Klinefelter syndrome
Definition
Klinefelter syndrome is a chromosome disorder in males that results in hypogonadism (small penis and small firm testicles). People with this condition are born with at least one extra X chromosome.
Description
Klinefelter syndrome is a condition where one or more extra X-chromosomes are present in a male. Boys with this condition appear normal at birth, but the defect becomes apparent in puberty when secondary sexual characteristics fail to develop, or develop later. By mid-puberty, boys with Klinefelter syndrome have low levels of testosterone, resulting in small testicles and the inability to make sperm. Affected males may also have learning disabilities and behavior problems such as shyness and immaturity and at an increased risk for certain other health problems such as pulmonary disease, varicose veins, breast cancer , extragonadal germ cell tumor (a rare tumor), and osteoporosis. Some mild cases may be undetected, with no abnormalities present except infertility.
Demographics
Klinefelter syndrome is one of the most common chromosomal abnormalities. About 1 in every 500 to 800 males is born with this disorder. Approximately 3% of the infertile male population have Klinefelter syndrome.
Causes and symptoms
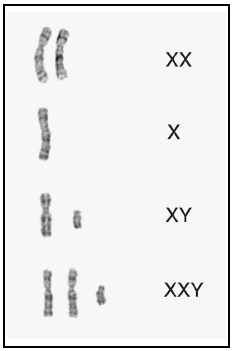
Normally, a person has a total of 46 chromosomes in each cell, two of which are responsible for determining that individual's sex. These two sex chromosomes are called X and Y. The combination of these two types of chromosomes determines the sex of a child. Females have two X chromosomes (the XX combination); males have one X and one Y chromosome (the XY combination).
In Klinefelter syndrome, a problem very early in fetal development results in an abnormal number of chromosomes. Most commonly, a male with Klinefelter syndrome will be born with 47 chromosomes in each cell, rather than the normal number of 46. The extra chromosome is an X chromosome. This means that rather than having the normal XY combination, the male has an XXY combination. Because people with Klinefelter syndrome have a Y chromosome, they are all male.
Approximately 1/3 of all males with Klinefelter syndrome have other chromosome changes involving an extra X chromosome. Mosaic Klinefelter syndrome occurs when some of the cells in the body have an extra X chromosome and the other have normal male chromosomes. These males can have the same or milder symptoms than those with non-mosaic Klinefelter syndrome. Males with more than one additional extra X chromosome, such as 48, XXXY, are usually more severely affected than males with 47,XXY.
Klinefelter syndrome is not considered an inherited condition. The risk of Klinefelter syndrome reoccurring in another pregnancy for a woman who had a son with Klinefelter syndrome is not increased above the risk of the general population.
The symptoms of Klinefelter syndrome are variable; not every affected person will have all of the features of the condition. Males with Klinefelter syndrome appear normal at birth and have normal male genitalia. From childhood, males with Klinefelter syndrome are taller than average with long limbs. Approximately 20–50% have a mild intention tremor, an uncontrolled shaking. Many males with Klinefelter syndrome have poor upper
Most boys enter puberty normally, though some can be delayed. The Leydig cells in the testicles usually produce testosterone. With Klinefelter syndrome, the Leydig cells fail to work properly causing the testosterone production to slow. By mid-puberty, testosterone production is decreased to approximately half of normal. This can lead to decreased facial and pubic hair growth. The decreased testosterone also causes an increase in two other hormones, follicle stimulating hormone (FSH) and luteinizing hormone (LH). Normally, FSH and LH help the immature sperm cells grown and develop. In Klinefelter syndrome, there are few or no sperm cells. The increased amount of FSH and LH cause hyalinization and fibrosis, the growth of excess fibrous tissue, in the seminiferous tubules, where the sperm are normally located. As a result, the testicles appear smaller and firmer than normal. With rare exception, men with Klinefelter syndrome are infertile because they can not make sperm.
While it was once believed that all boys with Klinefelter syndrome were mentally retarded, doctors now know that the disorder can exist without retardation. However, children with Klinefelter syndrome frequently have difficulty with language, including learning to speak, read, and write. Approximately 50% of males with Klinefelter syndrome are dyslexic. They may also have attention deficient hyperactivity disorder.
Some people with Klinefelter syndrome have difficulty with social skills and tend to be more shy, anxious, or immature than their peers. They can also have poor judgement and do not handle stressful situations well. As a result, they often do not feel comfortable in large social gatherings. Some people with Klinefelter syndrome can also have anxiety , nervousness and/or depression.
Taurodontism, an enlargement of the pulp of the teeth with surface thinning, is very common in Klinefelter syndrome and can be diagnosed with dental x rays.
The greater the number of X chromosomes present, the greater the disability. Boys with several extra X chromosomes have distinctive facial features, more severe retardation, deformities of bony structures, and even more disordered development of male features.
When to call the doctor
Parents should call a doctor if their son fails to develop secondary sexual characteristics at puberty.
Diagnosis
During a physical examination, a doctor will look for a simian crease (a single crease in the palm). A rectal exam may show an enlarged prostate. A single testicle may be present in the scrotum, indicating a probable undescended testicle. A semen examination will show low sperm count, while other tests will show decreased serum testosterone levels, increased levels of serum luteining and serum follicle stimulating hormones and increased serum estradiol levels (a type of estrogen).
Diagnosis of Klinefelter syndrome is confirmed by examining chromosomes for evidence of more than one X chromosome present in a male. This can be done in pregnancy with prenatal testing such as chorionic villus sampling or amniocentesis . Chorionic villus sampling is a procedure done early in pregnancy (approximately 10–12 weeks) to obtain a small sample of the placenta for testing. An amniocentesis is done further along in pregnancy (from approximately 16–18 weeks) to obtain a sample of fluid surrounding the baby for testing. Both procedures have a risk of miscarriage. Usually these procedures are done for a reason other than diagnosing Klinefelter syndrome. For example, a prenatal diagnostic procedure may be done on an older woman to determine if her baby has Down syndrome . If the diagnosis of Klinefelter syndrome is suspected in a young boy or adult male, chromosome testing can also be on a small blood or skin sample after birth.
Treatment
There is no treatment available to change chromosomal makeup. Children with Klinefelter syndrome may benefit from a speech therapist for speech problems or other educational intervention for learning disabilities. Testosterone injections started around the time of puberty and continued for life may help to produce more normal development, including more muscle mass, hair growth and increased sex drive. Testosterone supplementation will not increase testicular size, decrease breast growth or correct infertility.
Prognosis
While many men with Klinefelter syndrome live normal lives, nearly 100 percent of these men will be sterile (unable to produce a child). However, a few men with Klinefelter syndrome have been reported who have fathered a child through the use of assisted fertility services. Males with Klinefelter syndrome have an increased risk of several conditions such as osteoporosis, pulmonary disease, varicose veins, autoimmune disorders such as lupus and arthritis, diabetes, breast cancer and extragonadal germ cell tumor (a rare tumor).
Prevention
Klinefelter syndrome usually is not inherited but occurs during fetal development, so there is no means of preventing the disease. However, one risk factor for this condition is the mother giving birth at an older age; therefore, genetic counseling and testing is recommended.
Parental concerns
Families may wish to seek counseling regarding the effects of the syndrome on relationships within the family . Many people respond with guilt, fear , or blame when a genetic disorder is diagnosed in the family, or they may overprotect the affected member. Support groups are often good sources of information about Klinefelter syndrome; they can offer helpful suggestions about living with it as well as emotional support.
KEY TERMS
Follicle-stimulating hormone (FSH) —A pituitary hormone that in females stimulates the ovary to mature egg capsules (follicles) and in males stimulates sperm production.
Luteinizing hormone —A hormone secreted by the pituitary gland that regulates the menstrual cycle and triggers ovulation in females. In males it stimulates the testes to produce testosterone.
Testosterone —Male hormone produced by the testes and (in small amounts) in the ovaries. Testosterone is responsible for some masculine secondary sex characteristics such as growth of body hair and deepening voice. It also is sometimes given as part of hormone replacement therapy to women whose ovaries have been removed.
Resources
BOOKS
Bock, R. Understanding Klinefelter's Syndrome: A Guide for XXY Males and Their Families. Bethesda, MD: National Institutes of Health,1993.
Icon Health Publications. Klinefelter's Syndrome: A Medical Dictionary, Bibliography, and Annotated Research Guide to Internet References. San Diego, CA:Icon Health Publications, 2004.
Icon Health Publications. The Official Parent's Sourcebook on Klinefelter Syndrome. San Diego, CA:Icon Health Publications, 2002.
Probasco, Teri, and Gretchen A. Gibbs. Klinefelter Syndrome. Richmond, IN: Prinit Press, 1999.
ORGANIZATIONS
American Association for Klinefelter Syndrome Information and Support. 2945 West Farwell Avenue, Chicago, IL 60645-2925. (773) 761-5298, (800) 466-5747. http://www.aaksis.org
Klinefelter's Organisation. 234 Turton Road, Bolton, BL2 3EE, United Kingdom. http://www.klinefelter.org.uk/
Klinefelter Syndrome and Associates, Inc. PO Box 119, Roseville, CA 95678-0119. (916) 773-2999 or (888) 999-9428. Fax: (916) 773-1449. http://www.genetic.org/ks .
WEB SITES
Klinefelter Syndrome Support Group Home Page. http://klinefeltersyndrome.org/index.html
Judith Sims, MS Carin Lea Beltz, MS