Cleft lip and palate
Definition
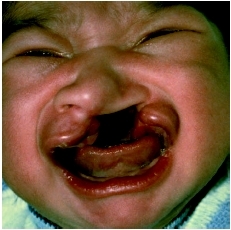
A cleft lip and/or palate is a birth defect (congenital) of the upper part of the mouth. A cleft lip creates an opening in the upper lip between the mouth and nose and a cleft palate occurs when the roof of the mouth has not joined completely.
Description
Cleft means split or separated. During the first months of pregnancy, separate areas of the face—such as bony and muscular parts, mouth, and throat, develop individually and then join together. If some parts do not join properly the result is a cleft, the type and severity of which can vary. During the fifth through ninth weeks of pregnancy genetic and environmental factors are most likely to affect lip and palate development. Cleft palate occurs when the right and left segments of the palate fail to join properly. The back of the palate (toward the throat) is called the soft palate, and the front section (toward the mouth opening) is known as the hard palate. A cleft palate can range from just an opening at the back of the soft palate to a nearly complete separation of the roof of the mouth (soft and hard palate). In some cases, an infant with a cleft palate may also have a small lower jaw and have difficulty breathing. This condition is called Pierre Robin sequence.
Cleft lip occurs when the lip elements fail to come together during fetal development, thus creating an opening in the upper lip between the mouth and nose. The lip looks split. A cleft lip may be complete, meaning that
Demographics
Over 5,000 infants are born each year in the United States with a cleft lip or palate (about one in every 700 births). Cleft lip without cleft palate is the third most common congenital malformation among newborns in the United States and is estimated to occur roughly twice as often in males than in females. Cleft palate without cleft lip is fifth most common, and it affects roughly twice as many girls as boys. Clefts may affect the left or right side of the mouth only (unilateral) or both sides (bilateral). Left-side clefts represent 70 percent of all unilateral clefts. In the United States, clefting seems to be at least in part related to ethnicity, occurring most often among Asians, Latinos, and Native Americans (one in 500), next most often among persons of European ethnicity (one in 700), and least often among persons of African ethnicity (one in 1,000).
Causes and symptoms
The causes of clefts are as of 2004 still poorly understood. Most scientists believe that clefting occurs as a result of a combination of genetic and environmental factors. In the United States and western Europe, researchers report that a family history of facial clefts is present in approximately 40 percent of all cases. The likelihood of a baby being born with a facial cleft increases if a first-degree relative (mother, father, or sibling) has a cleft. Mothers who abuse alcohol and drugs, lack vitamins (especially folic acid ) during the first weeks of pregnancy, or have diabetes are more likely to have a child with facial clefts.
Clefts may occur alone or with other abnormalities that may be hidden or obvious. Up to 13 percent of infants with cleft lip or palate have other birth defects. Some cases involve genetic syndromes that may result in specific problems for the infant and may have a high risk of affecting others in the family. For this reason, newborns with clefts should be thoroughly examined by a specialized physician soon after birth.
When to call the doctor
Families with a history of cleft lip or palate or any other syndrome or condition associated with clefting should discuss the chances of recurrence with a genetic counselor.
Diagnosis
Because clefting causes specific physical manifestations, it is easy to diagnose. Although some types of clefts can be detected during pregnancy by an ultrasound test, many are not discovered until birth.
Treatment
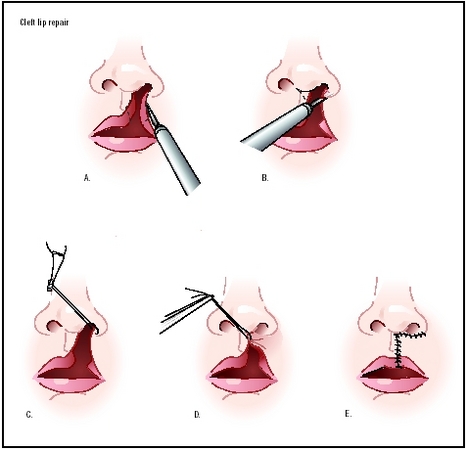
A cleft lip and/or palate can be repaired with corrective surgery, performed in a hospital under general anesthesia. Generally, within the first few days following birth of an infant with a facial cleft, a team is assembled to prepare a plan for treatment of the cleft. The treatment team usually includes representatives from several medical or psychological specialties, including pediatrics, plastic surgery, otolaryngology, orthodontia, prosthodontics, oral surgery, speech and language pathology, audiology, nursing, and psychology. It is common for one team member to coordinate service and communication between the team members and the family.
Surgical repair of a cleft lip is carried out at about three to four months of age. The whole emphasis in repairing the lip is on the muscle repair in order to mold the distorted front central section of the upper gum
Cleft palate can require several surgical procedures during the course of a child's first 18 years. The first surgery to repair the palate usually occurs when the infant is between six and 12 months old. It usually involves palatal lengthening and drawing tissue from either side of the mouth to rebuild the palate. The procedure usually requires two or three nights in the hospital, the first night in the intensive care unit. The purpose of this surgery is to create a functional palate, reduce the chances that fluid will develop in the middle ears, and help the proper development of the child's teeth and facial bones. In addition, the functional palate helps the child's speech development and feeding abilities. In both types of surgery, the necessity for more operations depends on the skill of the surgeon as well as the severity of the cleft, its shape, and the thickness of available tissue that can be used to create the palate. About 20 percent of children with a cleft palate require further surgical procedures to help improve their speech. Additional surgeries may also improve the appearance of the lip and nose, close openings between the mouth and nose, help breathing, and stabilize and realign the jaw.
Nutritional concerns
Infants with cleft lip or cleft soft palate generally have few feeding problems. However, when the cleft involves the hard palate, the infant is usually not able to suck efficiently. For these infants, caregivers must experiment with various feeding techniques, such as special nipples or alternate feeding positions. The infant with a cleft should be held in a nearly sitting position during feeding to prevent the breast or formula milk from flowing back into the nose. In addition, the infant should be burped frequently, approximately every three or four minutes. The sucking reflex is strong in all infants and should be encouraged in infants with facial clefts even if the sucking is inefficient, since the reflex seems to help the later development of speech. It is important to keep the cleft clean and not to allow formula, mucus, or other matter to collect in the cleft.
Prognosis
Both cleft lip and cleft palate are treatable birth defects. Most children born with either or both of these conditions undergo reconstructive surgery while they are still infants to correct the defect and significantly improve facial appearance. With advances in surgical techniques and with more complete repair of facial clefts, about 80 percent of affected children have normal speech development by the time they enter school. Continuation of speech therapy results in continuous improvement for most common speech problems.
Prevention
While little is known about how to prevent clefts, researchers from the California Birth Defects Monitoring Program found that women considering pregnancy may be able to reduce the risk of facial clefts (and possibly other birth defects) in their offspring by taking a multivitamin containing folic acid for one month prior to becoming pregnant. Other studies have shown that fetuses with certain predisposing genes may be at increased risk for cleft palate if their mothers smoke. Because some types of medications (for example some drugs used to treat epilepsy) have been linked to increased risk of clefts, women who take medications for chronic illnesses should check with their doctors before they become pregnant.
Parental concerns
Parents of a newborn baby with a cleft lip or palate are often confused and afraid of the impact the defect will have on their child's life. These feelings can be alleviated by learning about the cleft and treatment options. They also must communicate what they are learning about clefts to family, siblings, and friends. It is important for people who come into contact with the child to realize that a cleft is not a wound, although it may give the impression that it is tender or sore. Parents can help others understand that the cleft does not hurt and that it will be repaired. To ensure normal psychological and speech development, parents should interact with their infant as they would with any newborn in the family and should encourage others to do the same.
KEY TERMS
Bilateral cleft lip —A cleft that occurs on both sides of the lip.
Cleft —An elongated opening or slit in an organ.
Complete cleft —A cleft that extends through the entire affected mouth structure.
Congenital —Present at birth.
Palatal lengthening (palatal pushback) —A surgical procedure in which tissue from the front part of the mouth is moved back to lengthen it.
Palate —The roof of the mouth.
Premaxilla —The front central section of the upper gum, containing the four upper front teeth.
Unilateral cleft —A cleft that occurs on only the right or left side of the lip.
As the child with a cleft grows and develops, he or she will certainly experience many good and bad reactions from adults and children. Other children may tease the child or use the term "harelip." It may be helpful for parents of a child with a facial cleft to meet with his classmates and teachers to explain the history of the term harelip. Although a facial cleft was once referred to as a harelip to reflect its similarity to the mouth of a rabbit, the term is considered insulting today. Educating adults and children about cleft lip and palate is the best way to relieve others' anxiety about the defect and lessen any negative psychological effects that bad reactions might have on the child.
See also Language development .
Resources
BOOKS
Bzoch, Kenneth R. Communicative Disorders Related to Cleft and Lip Palate. Austin, TX: PRO-ED Inc., 2004.
Golding-Kushner, Karen J. Therapy Techniques for Cleft Palate Speech and Related Disorders. San Diego, CA: Singular Publishing Group Inc., 2001.
Gruman-Trinkner, Carrie, and Blaise Winter. Your Cleft-Affected Child: The Complete Book of Information, Resources, and Hope. Berkeley, CA: Publishers Group West, 2001.
Wysznski, Diego I. Cleft Lip and Palate: From Origin to Treatment. Oxford, UK: Oxford University Press, 2002.
PERIODICALS
Caniklioglu, M. C. "Use of a nickel titanium palatal expander in cleft-palate cases." Journal of Clinical Orthodontics 38, no. 7 (July 2004): 374–77.
Chapman, K. L. "Is presurgery and early postsurgery performance related to speech and language outcomes at 3 years of age for children with cleft palate?" Clinical Linguistics and Phonetics 18, no. 4–5 (June-August 2004): 235–57.
Hermann, N. V., et al. "Early craniofacial morphology and growth in children with bilateral complete cleft lip and palate." Cleft Palate and Craniofacial Journal 41, no. 4 (July 2004): 104–05.
Mulliken, J. B. "The changing faces of children with cleft lip and palate." New England Journal of Medicine 351, no. 8 (August 2004): 745–47.
Smith, A. S., et al. "Prenatal diagnosis of cleft lip and cleft palate using MRI." American Journal of Roentgenology 183, no. 1 (July 2004): 229–35.
Van Lierde, K. M., et al. "Vocal quality characteristics in children with cleft palate: a multiparameter approach." Journal of Voice 18, no. 3 (September 2004): 354–62.
Whitehill, T. L., and C. H. Chau. "Single-word intelligibility in speakers with repaired cleft palate." Clinical Linguistics and Phonetics 18, no. 4–5 (June-August 2004): 341–55.
ORGANIZATIONS
About Face USA. PO Box 969, Batavia, IL 60510–0969. Web site: http://www.aboutfaceusa.org/default.htm.
American Cleft Palate: Craniofacial Association (ACPCA)/Cleft Palate Foundation (CPF). 1504 East Franklin Street, Suite 102, Chapel Hill, NC 27514–2820. Web site: http://www.cleftline.org.
American Speech-Language-Hearing Association. 10801 Rockville Pike, Rockville, MD 20852. Web site: http://www.asha.org.
Children's Craniofacial Association (CCA). 13140 Coit Road, Suite 307, Dallas, Texas 75240. Web site: http://www.ccakids.org/default.htm.
WEB SITES
"Cleft Lip and Palate Resource." Wide Smiles. Available online at http://www.widesmiles.org (accessed November 16, 2004).
March of Dimes Homepage. Available online at http://www.modimes.org/ (accessed November 15, 2004).
Monique Laberge, Ph.D.
if their parents is relative,is their chance of getting this abnormalities is higher?(without any history of relative having this cleft palate and lip)if yes,why?