Cesarean section
Definition
A cesarean section (also referred to as c-section) is the birth of a fetus accomplished by performing a surgical incision through the maternal abdomen and uterus. It is one of the oldest surgical procedures known throughout history.
Purpose
Although Healthy People 2010 established a goal of a 15 percent rate for c-sections in the United States, the ideal rate has not been established. As of 2004, the average c-section rate is one out of every four births or approximately 26 percent of all births. A c-section allows safe and quick delivery of a baby when a vaginal delivery is not possible. The surgery is performed in the presence of a variety of maternal and fetal conditions with the most commonly accepted indications being complete placenta previa, cephalopelvic disproportion (CPD), placental abruption, active genital herpes, umbilical cord prolapse, failure to progress in labor or dystocia, proven nonreassuring fetal status, and benign and malignant tumors that obstruct the birth canal. Indications that are more controversial include breech presentation, previous c-section, major congenital anomalies, cervical cerclage, and severe Rh isoimmunization. C-sections have a higher maternal mortality rate than vaginal births with approximately 5.8 women per 100,000 live births dying, and half of these deaths are ascribed to the operation and a coexisting medical condition. Perinatal morbidity is associated with infections, reactions to anesthesia agents, blood clots, and bleeding.
Description
According to the United States Public Health Service, 35 percent of all c-sections are performed because the woman has had a previous c-section. The skin incision for a c-section is either transverse (Pfannenstiel) or vertical and does not indicate the type of incision made into the uterus. "Once a cesarean, always a cesarean," is a rule that originated with the classical, vertical uterine incision. It was believed that the resulting scar weakened the uterus wall and was at risk of rupture in subsequent deliveries. As of 2004, the incision is almost always made horizontally across the lower uterine segment, called a low transverse incision. This results in reduced blood loss and a decreased chance of rupture. This kind of incision allows many women to have a vaginal birth after a cesarean (VBAC).
Failure to progress and/or dystocia is the second most common reason for a c-section and represents about 30 percent of all cases. Uterine contractions may be weak or irregular, the cervix may not be dilating, or the mother's pelvic structure may not allow adequate passage for birth. When the baby's head is too large to fit through the pelvis, the condition is called cephalopelvic disproportion (CPD). Failure to progress, however, can only be diagnosed with documentation of adequate contraction strength. The force of the contractions can be measured with an intrauterine pressure catheter (IUPC), which is a catheter that can be placed through the cervix into the uterus to measure uterine pressure during labor. Calculation of this force is determined by subtracting the baseline (resting) pressure from the peak pressure recorded for all contractions in a ten-minute period. This pressure calculation results in a force termed Montevideo units. A minimum of 200 Montevideo units are required before the forces of labor can be considered adequate. If the Montevideo units are less than this ten-minute sum and the fetal heart rate is reassuring, augmentation of labor with pitocin may be necessary.
Breech presentation occurs in about 3 percent of all births, and approximately 12 percent of c-sections are performed to deliver a baby in a breech presentation: buttocks or feet first. Breech presentations were still delivered vaginally in the 1970s, but with the advent of the malpractice climate, many doctors shied away from this practice, opting to perform a c-section. As a result, physicians who were being trained during that time period never learned how to manage a breech vaginal delivery. There was some change in this approach in the 1990s, and doctors are once again learning how to manage this situation; however, it is still uncertain whether this knowledge will be used in their practice.
Fetal distress or the more appropriate term, nonreassuring fetal heart rate, accounts for almost 9 percent of c-sections. With the introduction of electronic fetal monitoring (EFM) in the 1970s, doctors had more information for assessing fetal well-being. It was assumed that fetal monitoring would transmit signals of distress, thus, the EFM tracing became a legal document. There is still considerable debate as to what a non-reassuring FHR really is, but there are other parameters available to assist in this interpretation. When a fetus experiences stress, (oxygen deprivation) in utero, it may pass meconium (feces) into the amniotic fluid. The appearance of meconium in the fluid along with a questionable EFM tracing may indicate that a fetus is becoming compromised. At this point, if a woman is in early labor, a c-section may have to be performed. If, however, she is close to delivery, a vaginal delivery is often quicker. Oxygen deprivation may also be determined by testing the pH of a blood sample taken from the baby's scalp: a pH of 7.25-7.35 is normal; between 7.2 and 7.25 is suspicious; and below 7.2 is a sign of trouble. If the sample is equivocal, it can be repeated every 20 to 30 minutes.
The remaining 14 percent of c-sections occur secondary to other emergency situations, including the following:
- Umbilical cord prolapse: This situation occurs when the cord is the presenting part from the vagina. It becomes compressed and cuts off blood flow to the baby. The birth attendant must insert a hand into the vagina and relieve pressure on the cord until a c-section is performed.
- Placental abruption: The placenta separates from the uterine wall before the baby is born. If it is a complete abruption, the baby's blood flow will be cut off completely. The mother experiences severe pain , possible bleeding, and her abdomen feels rock hard. This situation demands an immediate c-section. Partial abruptions can occur without endangering the mother or the baby, but they need to be closely monitored. The risk of placental abruption is higher in multiple births and in women with high blood pressure.
- Placenta previa: With a complete previa, the placenta covers the cervix completely, and the mother may experience painless bleeding. With a complete previa, a c-section is mandatory as cervical dilation would cause bleeding. The baby is often in a transverse position in this case, which means it is lying horizontally across the pelvis. Women with partial previas will usually need a c-section due to bleeding problems, but those with marginal previas can often deliver vaginally.
- Active genital herpes: Any active herpetic lesions in the vaginal area can infect the baby as it passes through the birth canal. This is especially true for those with a primary outbreak, a first-time exposure.
- Mother's health status: A c-section may be necessary in women with pre-existing diseases, such as diabetes, hypertension , pregnancy induced hypertension (preeclampsia), autoimmune diseases such as lupus erythematosus, and blood incompatibilities. Each case must be evaluated on an individual basis in these instances to achieve the optimal outcome for baby and mother.
Precautions
There are some precautions any pregnant woman can follow to enhance her chances of preventing a c-section. These include the following:
- She should check her doctor's c-section rate to see if it is unnecessarily high. She can ask what his/her rate is and verify it by checking with the labor and delivery nurses at the hospital or with a childbirth educator.
- She should not stay on her back during labor. She can walk, rock, or use a hot shower or whirlpool.
- From the beginning, she should discuss with her doctor that she wants to avoid having a c-section if at all possible and enlist his opinion on how to achieve it.
- Studies show that women who go to the hospital early have a higher c-section rate than those who do not. Therefore, when labor starts, the woman should stay home for as long as she safely can. She should not go in if contractions are further apart than four to five minutes.
- She should use a midwife since studies show that they have a higher percentage of natural childbirths without surgical intervention than obstetricians do.
- She should hire a doula to assist during labor birth. Doulas have a lower c-section rate and can offer massage, different positions, and support alternatives during the difficult phases of labor.
- She should gather as much information as possible on hospital policies to educate herself and then discuss this information with her doctor or midwife. She should keep an open mind and stay informed.
Preparation
There is no perfect anesthesia for a c-section because every choice has its advantages and disadvantages. When a c-section becomes necessary and if it is not an emergency, the mother and her significant other should take part in the choice of anesthetic by being informed of risks and side effects. The anesthesia is usually a regional anesthetic (epidural or spinal), which makes her numb from below her breasts to her toes. In some cases, a general anesthetic will be administered if the regional does not work or if it is an emergency c-section. Every effort should be made to include the significant other in the preparations and recovery as well as the surgery if at all possible. An informed consent needs to be signed, and the physician should explain the surgery at that time. The mother may already have an intravenous (IV) line of fluid running into a vein in her arm. A catheter is inserted into her bladder to keep it drained and out of the way during surgery and the upper pubic area is usually shaved. Antacids are frequently administered to reduce the likelihood of damage to the lungs should aspiration of gastric contents occur. The abdominal area is then scrubbed and painted with betadine or another antiseptic solution. Drapes are placed over the surgical area to block a direct view of the procedure.
The type of skin incision, transverse or vertical, is determined by time factor, preference of mother, or physician preference. Two major locations of uterine incisions are the lower uterine segment and the upper segment of the body of the uterus (classical incision). The most common lower uterine segment incision is a transverse incision because the lower segment is the
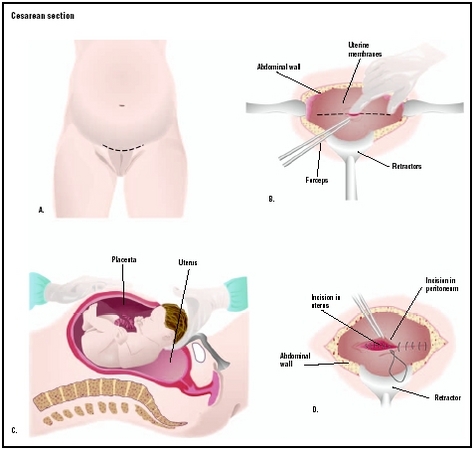
Once the uterus is opened, the amniotic sac is ruptured and the baby is delivered. The time from the initial incision to birth is typically five to ten minutes. The umbilical cord is clamped and cut, and the newborn is given to the nursery personnel for evaluation. Cord blood is normally obtained for analysis of the infant's blood type and pH. The placenta is removed from the mother and her uterus is closed with suture. The abdominal area may be closed with suture or surgical staple. The time from birth through suturing may take 30 to 40 minutes. The entire surgical procedure may be performed in less than one hour. Physical contact or

Aftercare
Immediate postpartal care after a c-section is similar to post-operative care with the exception of palpating the fundus (top of the uterus) for firmness. If an epidural or spinal were used, Duramorph (a pain medication similar to morphine) is often administered through these catheters just prior to completion of surgery. It does very well in controlling pain but may cause itching , which can be managed. During recovery the mother is encouraged to turn, cough , and deep breathe to keep her lungs clear, and the neonate is usually brought to the mother to breastfeed if she so desires. The mother will be encouraged to get out of bed about eight to 24 hours after surgery. Walking stimulates the circulation to avoid formation of blood clots and promotes bowel movement. Once discharged home, the mother should limit stair climbing to once a day, and she should avoid lifting anything heavier than the baby. It is important to nap as often as the baby does and make arrangements for help with the housework, meals, and care of other children. Driving may be resumed after two weeks, although some doctors recommend waiting for six weeks, which is the typical recovery period from major surgery.
Risks
The maternal death rate for c-section is less than 0.02 percent (5.8 per 100,000 live births), but that is four times the maternal death rate associated with vaginal delivery. The mother is at risk for increased bleeding from two incision sites and a c-section usually has twice as much blood loss as a vaginal delivery during surgery. Complications occur in less than 10 percent of cases, but these complications can include an infection of the incision, urinary tract, or tissue lining the uterus (endometritis). Less commonly, injury can occur to the surrounding organs, i.e., the bladder and bowel.
Normal results
The after-effects of a c-section vary, depending on the woman's age, physical fitness, and overall health. Following this procedure, a woman commonly experiences gas pains, incision pain, and uterine contractions, which are also common with vaginal delivery. The hospital stay may be three to four days. Breastfeeding the baby is encouraged, taking care that it is in a position that keeps the baby from resting on the mother's incision. As the woman heals, she may gradually increase appropriate exercises to regain abdominal tone. Full recovery may be seen in four to six weeks.
The prognosis for a successful vaginal birth after a cesarean (VBAC) may be at least 75 percent, especially when the c-section involved a low transverse incision in the uterus, and there were no complications during or after delivery.
Of the hundreds of thousands of women in the United States who undergo a c-section each year, about 500 die from serious infections, hemorrhaging, or other complications. These deaths may be related to the health conditions that made the operation necessary and not simply to the operation itself.
Parental concerns
Undergoing a c-section may inflict psychological distress on the mother, beyond hormonal mood swings and postpartum depression. The woman may feel disappointment and a sense of failure for not experiencing a vaginal delivery. She may feel isolated if the father or birthing coach is not with her in the operating room or if she is treated by an unfamiliar doctor rather than by her own doctor or midwife. She may feel helpless from a loss of control over labor and delivery with no opportunity to actively participate. To overcome these feelings, the woman needs to understand why the c-section was crucial. It is important that she be able to verbalize an understanding that she could not control the events that made the c-section necessary and recognize the importance of preserving the health and safety of both herself and her child. Women who undergo a c-section should be encouraged to share their feelings with others. Hospitals can often recommend support groups for such mothers. Women should also be encouraged to seek professional help if negative emotions persist.
KEY TERMS
Breech presentation —The condition in which the baby enters the birth canal with its buttocks or feet first.
Cephalopelvic disproportion —The condition in which the baby's head is too large to fit through the mother's pelvis.
Cervical cerclage —A procedure in which the cervix of the uterus is sewn closed, it is used in cases when the cervix starts to dilate too early in a pregnancy to allow the birth of a healthy baby.
Doula —A doula is someone who undergoes special training to enable them to support women during childbirth and into the postpartum period.
Dystocia —Failure to progress in labor, either because the cervix will not dilate (expand) further or because the head does not descend through the mother's pelvis after full dilation of the cervix.
Genital herpes —A life-long, recurrent sexually transmitted infection caused by the herpes simplex virus (HSV).
Perinatal —Referring to the period of time surrounding an infant's birth, from the last two months of pregnancy through the first 28 days of life.
Pitocin —A synthetic hormone that produces uterine contractions.
Placenta previa —A condition in which the placenta totally or partially covers the cervix, preventing vaginal delivery.
Placental abruption —An abnormal separation of the placenta from the uterus before the birth of the baby, with subsequent heavy uterine bleeding. Normally, the baby is born first and then the placenta is delivered within a half hour.
Postpartal —The six-week period following childbirth.
Rh blood incompatibility —Incompatibility between the blood of a mother and her baby due the absence of the Rh antigen in the red blood cells of one and its presence in the red blood cells of the other.
Umbilical cord prolapse —A birth situation in which the umbilical cord, the structure that connects the placenta to the umbilicus of the fetus to deliver oxygen and nutrients, falls out of the uterus and becomes compressed, thus preventing the delivery of oxygen.
See also Apgar testing ; Electronic fetal monitoring .
Resources
BOOKS
Olds, Sally et al. Maternal-Newborn Nursing & Women's Health Care , 7th ed. Saddle River, NJ: Prentice Hall, 2004.
ORGANIZATIONS
Association of Women's Health, Obstetric and Neonatal Nursing. 2000 L Street, NW, Suite 740, Washington, DC 20036. Web site: http://www.awhonn.org.
International Childbirth Education Association Inc. (ICEA). PO Box 20048, Minneapolis, MN 55420. Web site: http://www.icea.org/info.htm.
WEB SITES
"Cesarean Section." MedlinePlus. Available online at http://www.nlm.nih.gov/medlineplus/cesareansection.html (accessed December 7, 2004).
"Cesarean Section Homepage." Childbirth. Available online at http://www.childbirth.org/section/section.html (accessed December 7, 2004).
"C-Section." March of Dimes. Available online at http://www.marchofdimes.com/pnhec/240_1031.asp (accessed December 7, 2004).
Linda K. Bennington, RNC, MSN, CNS