Scoliosis
Definition
Scoliosis is a side-to-side curvature of the spine.
Description
When viewed from the rear, the spine usually appears perfectly straight. Scoliosis is a lateral (side-to-side) curve in the spine, usually combined with a rotation of the vertebrae. (The lateral curvature of scoliosis should not be confused with the normal set of front-to-back spinal curves visible from the side.) While a small degree of lateral curvature does not cause any medical problems, larger curves can cause postural imbalance and lead to muscle fatigue and pain . More severe scoliosis can interfere with breathing and lead to arthritis of the spine (spondylosis).
Demographics
Approximately 10 percent of all adolescents have some degree of scoliosis, although fewer than 1 percent have curves that require medical attention beyond monitoring. Scoliosis is found in both boys and girls, but a girl's spinal curve is much more likely to progress than a boy's. Girls require scoliosis treatment about five times more often than boys. The reason for these differences as of 2004 was not known.
Causes and symptoms
Four out of five cases of scoliosis are idiopathic, meaning the cause is unknown. While idiopathic scoliosis tends to run in families, no specific genes responsible for the condition have been identified. Children with idiopathic scoliosis appear to be otherwise entirely healthy and have not had any bone or joint disease early in life. Scoliosis is not caused by poor posture, diet, or carrying a heavy book bag on one shoulder.
Idiopathic scoliosis is further classified according to age of onset:
- Infantile: Curvature appears before age three. This type is quite rare in the United States but is more common in Europe.
- Juvenile: Curvature appears between ages three and ten. This type may be equivalent to the adolescent type, except for the age of onset.
- Adolescent: Curvature usually appears between ages of ten and 13, near the beginning of puberty . This is the most common type of idiopathic scoliosis.
- Adult: Curvature begins after physical maturation is completed.
Causes are known for three other types of scoliosis:
- Congenital scoliosis is due to abnormal formation of the bones of the spine and is often associated with other organ defects.
- Neuromuscular scoliosis is due to loss of control of the nerves or muscles that support the spine. The most common causes of this type of scoliosis are cerebral palsy and muscular dystrophy .
- Degenerative scoliosis may be caused by breaking down of the discs that separate the vertebrae or by arthritis in the joints that link them.
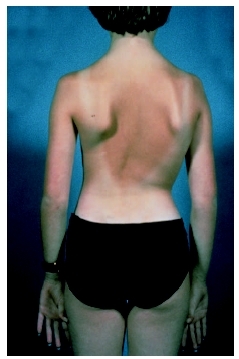
Scoliosis causes a noticeable asymmetry in the torso when viewed from the front or back. The first sign of scoliosis is often seen when a child is wearing a bathing suit or underwear. A child may appear to be standing with one shoulder higher than the other or to have a tilt in the waistline. One shoulder blade may appear more prominent than the other due to rotation. In girls, one breast may appear higher than the other or larger if rotation pushes one side forward.
Curve progression is greatest near the adolescent growth spurt. Scoliosis that begins early is more likely to progress significantly than scoliosis that begins later in puberty.
When to call the doctor
If the parent notices that a child's posture is abnormal, if when the child stands one hip appears to be higher than the other, if one shoulder blade appears to be sticking out, or the child appears to lean regularly to one side, the doctor should be notified. If the child is screened at school and the screener reports a suspicion of scoliosis, a doctor should be seen to follow up on this suspicion.
Diagnosis
Diagnosis for scoliosis is done by an orthopedist. A complete medical history is taken, including questions about family history of scoliosis. The physical examination includes determination of pubertal development in adolescents, a neurological exam (which may reveal a neuromuscular cause), and measurements of trunk asymmetry. Examination of the trunk is done while the patient is standing, bending over, and lying down and involves both visual inspection and use of a simple mechanical device called a scoliometer.
If a curve is detected, one or more x rays will usually be taken to define the curve or curves more precisely. An x ray is also used to document spinal maturity, any pelvic tilt or hip asymmetry, and the location, extent, and degree of curvature. The curve is defined in terms of where it begins and ends, in which direction it bends, and by an angle measure known as the Cobb angle. The Cobb angle is found by taking an x ray of the spine. Lines are then projected out parallel to the vertebrae at the top and bottom of the curve. Then perpendicular lines are projected from these lines and the angle at which the lines intersect is measured. These angles are referred to when the angle of the curvature is discussed. To properly track the progress of scoliosis, it is important to project from the same points of the spine each time a measurement is made; otherwise, there is a risk of getting misleading measurements.
Occasionally, magnetic resonance imaging (MRI) is used as a diagnostic tool, primarily to look more closely at the condition of the spinal cord and nerve roots extending from it if neurological problems are suspected.
Treatment
Treatment decisions for scoliosis are based on the degree of curvature, the likelihood of significant progression, and the presence of pain, if any.
Curves less than 20 degrees are not usually treated, except by regular follow-up for children who are still growing. Watchful waiting is usually all that is required in adolescents with curves of 20 to 30 degrees as long as there is no pain.
For children or adolescents whose curves progress to 30 degrees and who have a year or more of growth left, bracing may be required. Bracing cannot correct curvature but may be effective in halting or slowing progression.
Two styles of braces are used for daytime wear. The Milwaukee brace consists of metal uprights attached to pads at the hips, rib cage, and neck. The other kind of brace is the underarm brace, which uses rigid plastic to encircle the lower rib cage, abdomen, and hips. Both these brace types hold the spine in a vertical position. Because it can be worn out of sight beneath clothing, the underarm brace is better tolerated and often leads to better compliance. A third style, the Charleston bending brace, is used at night to bend the spine in the opposite direction. Braces are often prescribed to be worn for 22 to 23 hours per day, though some clinicians allow or encourage removal of the brace for exercise .
Bracing may be appropriate for scoliosis due to some types of neuromuscular disease, including spinal muscular atrophy , before growth is finished. Duchenne muscular dystrophy is not treated by bracing. Surgery is likely to be required.
Surgery is usually the option of last resort in cases of scoliosis. Surgery for idiopathic scoliosis is usually recommended if one of the following conditions is present:
- The curve has progressed despite bracing.
- The curve is greater than 40 to 50 degrees before growth has stopped in an adolescent.
- There is significant pain.
Orthopedic surgery for neuromuscular scoliosis is often done earlier. The goals of surgery are to correct the deformity as much as possible, to prevent further deformity, and to eliminate pain as much as possible. Surgery can usually correct 40 to 50 percent of the curve, and sometimes as much as 80 percent. Surgery cannot always completely remove pain.
The surgical procedure for scoliosis is called spinal fusion, because the goal is to straighten the spine as much as possible and then to fuse the vertebrae together to prevent further curvature. To achieve fusion, the involved vertebra are first exposed and then scraped to promote regrowth. Bone chips are usually used to splint together the vertebrae to increase the likelihood of fusion. To maintain the proper spinal posture before fusion occurs, metal rods are inserted alongside the spine and are attached to the vertebrae by hooks, screws, or wires. Fusion of the spine makes it rigid and resistant to further curvature. The metal rods are no longer needed once fusion is complete but are rarely removed unless their presence leads to complications.
Spinal fusion leaves the involved portion of the spine permanently stiff and inflexible. While this leads to some loss of normal motion, most functional activities are not strongly affected, unless the very lowest portion of the spine (the lumbar region) is fused. Normal mobility, exercise, and even contact sports are usually all possible after spinal fusion. Full recovery takes approximately six months. Physical therapy is part of standard treatment as well.
Alternative treatment
Numerous alternative therapies have been touted to provide relief and help for individuals with scoliosis, but none has been proven beneficial in clinical trials. These include massage and electrical stimulation. In addition, alternatives such as rolfing or chiropractic manipulation of soft tissue to improve alignment may provide improved flexibility, stronger muscles, and pain relief but cannot prevent or correct the curvature of the spine or its progression.
Although important for general health and strength, exercise has not been shown to prevent or slow the development of scoliosis. It may help relieve pain from scoliosis by helping to maintain range of motion. Aquatic exercise, in particular, can increase flexibility and improve posture, balance, coordination, and range of motion. Because it decreases joint compression, it can lessen the pain caused by scoliosis or surgery.
Good nutrition is also important for general health, but no specific dietary regimen has been shown to control scoliosis development. In particular, dietary calcium levels do not influence scoliosis progression.
Chiropractic treatment may relieve pain, but it cannot halt scoliosis development and should not be a substitute for conventional treatment of progressing scoliosis. Acupuncture and acupressure may also help reduce pain and discomfort, but these treatments cannot halt scoliosis development either.
Prognosis
The prognosis for a child with scoliosis depends on many factors, including the age at which scoliosis begins and the treatment received. More importantly, mostly unknown individual factors affect the likelihood of progression and the severity of the curve. Most cases of mild adolescent idiopathic scoliosis need no treatment and do not progress. Untreated severe scoliosis often leads to spondylosis and may impair breathing. Degenerative arthritis of the spine, sciatica, and severe physical deformities can also result if severe scoliosis is left untreated. Finally, scoliosis can also poorly affect the individual's self-esteem and cause serious emotional problems.
Prevention
There is no known way to prevent the development of scoliosis. Progression of scoliosis may be prevented through bracing or surgery. More than 30 states have screening programs in schools for adolescent scoliosis, usually conducted by trained school nurses or physical education teachers. These programs can help to catch scoliosis early, so that treatment can begin and progression can often be halted or slowed.
Parental concerns
Children with scoliosis often have a negative self-image associated with irregular posture or having to wear a brace. This problem is being combated with new braces that can be worn under the clothing and are more discreet than traditional braces. Scoliosis can be life threatening if it is not treated and progresses to a point at which breathing is impaired. This is very rare, however.
Resources
BOOKS
Hooper, Nancy J. Stopping Scoliosis: The Whole Family Guide to Diagnosis and Treatment. East Rutherford, NJ: Penguin Group, 2002.
Lenke, Lawrence, et al. Modern Anterior Scoliosis Surgery. St. Louis, MO: Quality Medical Publishing, 2002.
Newton, Peter O. Adolescent Idiopathic Scoliosis. Rosemont, IL: Academy of Orthopaedic Surgeons, 2004.
Schommer, Nancy. Stopping Scoliosis: The Complete Guide to Diagnosis and Treatment , 2nd ed. New York: Avery, 2002.
Silverstein, Alvin. Scoliosis. Minneapolis, MN: Sagebrush Education Resources, 2003.
Spray, Michelle L., et al. Growing Up with Scoliosis: A Young Girl's Story. Stratford, CT: Book Shelf Inc., 2002.
PERIODICALS
Sullivan, Michele G. "Surgical Stapling Can Halt Curve of Scoliosis: Orthotics Can Be Helpful." Family Practice News 33 (December 15, 2003): 35.
Wachter, Kerry. "Prognosis for Scoliosis Better than Once Thought." Family Practice News 33 (July 1, 2003): 59.
Weomstoem. Stuart, et al. "Health and Function of Patients with Untreated Idiopathic Scoliosis: a 50-Year Natural History Study." The Journal of the American Medical Association 289 (February 5, 2003): 559.
ORGANIZATIONS
National Scoliosis Foundation. 5 Cabot Place, Stoughton, MA 02072. Web site: http://www.scoliosis.org.
Scoliosis Research Society. 55 East Wells St. Suite 1100. Milwaukee, WI 53202–3823. Web site: http://www.srs.org.
Tish Davidson, A.M. Liz Meszaros
KEY TERMS
Cobb angle —A measure of the curvature of scoliosis, determined by measurements made on x rays.
Rolfing —A holistic system of bodywork that uses deep manipulation of the body's soft tissue to realign and rebalance the body's myofacial (connective) structure. It is used to improve posture, relieve chronic pain, and reduce stress.
Comment about this article, ask questions, or add new information about this topic: