Otitis media

Definition
Otitis media is an infection of the middle ear, which is located behind the eardrum. There are two main types of otitis media. In the first, called acute otitis media (AOM), parts of the ear are infected and swollen, and fluid and mucus are trapped inside the ear. AOM can be quite painful. In the second type, called otitis media with effusion (fluid), or OME, fluid and mucus remain trapped within the ear after the infection is over, making it more difficult for the ear to fight off new infections. This fluid may adversely affect a child's hearing.
Description
One of the most common childhood infections, Otitis media is the leading cause of visits to the doctor by children. It is also the most frequent reason children receive antibiotic prescriptions or undergo surgery.
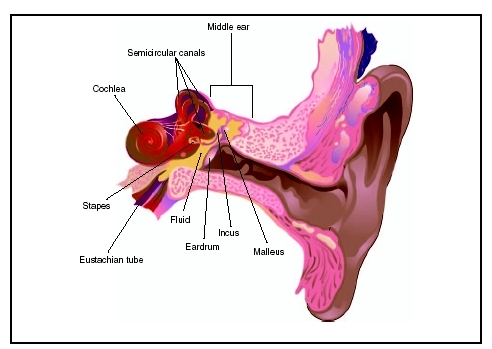
In order to fully understand otitis media, it is helpful to have a basic knowledge of ear anatomy. Deep within the outer ear canal is the eardrum, which is a thin, transparent membrane that vibrates in response to sound. Behind the eardrum is the space called the middle ear. When the eardrum vibrates, three tiny bones within the middle ear, called ossicles, transmit these sounds to the inner ear. Nerves are stimulated in the inner ear, which then relay the sound signals to the brain. The eustachian tube, which connects the middle ear to the nose, normally equalizes pressure in the middle ear, allowing the eardrum and ossicles to vibrate correctly, so that hearing is normal.
There are certain factors particular to children that make them more at risk for otitis media. In children, the eustachian tube is shorter and less slanted than in adults. Its size and position allow bacteria and viruses to travel to the middle ear more easily. Children also have clumps of infection fighting cells, commonly called adenoids, in the area of the eustachian tube. These adenoids may enlarge with repeated respiratory tract infections and ultimately block the eustachian tubes. When these tubes are blocked, the middle ear is more likely to fill with fluid, which in turn increases the risk for infection.
Demographics
Otitis media is common. Fifty percent of children have an episode before their first birthday, and 80 percent of children have an occurrence by their third birthday. It is estimated that $3 to $4 billion are spent per year on patients with a diagnosis of acute otitis media and related complications. Ear infections are found in all age groups, but they are considerably more common in children, especially those aged six months to three years. Boys are affected more commonly than girls. Other children at higher risk include those from poor families, Native Americans, children born with cleft palate or other defects of the facial structures, and children with Down syndrome . Exposure to cigarette smoke and early entrance into daycare also increase the risk. Otitis media occurs more frequently in winter and early spring. It is less common among children who are breastfeeding. Some studies show a genetic predisposition towards developing otitis media.
Causes and symptoms
The first precondition for the development of acute otitis media is exposure to an organism capable of causing the infection. Otitis media may be caused by either viruses or bacteria. Viral infections account for approximately 15 percent of cases. The majority of other cases are caused by a variety of bacteria. The three most common bacteria are Streptococcus pneumoniae (responsible for 25–50% of cases), Haemophilus influenzae (15–30%), and Moraxella catarrhalis (3–20%).
Acute otitis media often occurs as an aftereffect of upper respiratory infections, in which the eustachian tube and nasal membranes become swollen and congested. This condition can lead to an impaired clearance and pressure regulation in the middle ear, which, if sustained, may be followed by viruses and bacteria traveling from the nasopharynx to the middle ear.
Otitis media with effusion may develop within weeks of an acute episode of middle ear infection, but in many cases the cause is unknown. It is often associated with an abnormal or malfunctioning eustachian tube, which causes negative pressure in the middle ear and leaking of fluid from tiny blood vessels, or capillaries, into the middle ear.
Symptoms of acute otitis media (AOM)
The following are symptoms of acute otitis media:
- fever
- ear pulling
- complaints of ear pain , ear fullness, or hearing loss by older children
- fussiness, irritability, or difficulties in hearing, feeding, or sleeping in younger children
- bloody or greenish-yellow pus draining from the ear (This seepage is the sign of a perforated the eardrum. The pain leading up to such a perforation may be severe, but it is often relieved by the rupture.)
Otitis media with effusion (OME) is the presence of middle ear fluid for six weeks or longer after the initial episode of acute otitis media. The hallmark of OME is the lack of obvious symptoms in those who most commonly have the condition. Older children often complain of muffled hearing or a sense of fullness in the ear. Younger children may turn up the television volume. Most often OME is diagnosed when someone examines the ear for another reason, such as a well-child physical. For this reason, OME is often referred to as silent otitis media.
When to call the doctor
Unresolved episodes of otitis media may lead to a variety of complications, including hearing loss and dizziness . Any child who reports an earache or a sense of fullness in the ear, especially if combined with a prior upper respiratory tract infection, or fever, should be evaluated by a physician.
Diagnosis
The physician will visualize the ear canal and ear drum by using a special lighted instrument called an otoscope. Normally, the light from the otoscope reflects off the eardrum in a characteristic fashion called the "cone of light." In an infection, this reflection is often shifted or absent. If fluid or pus is draining from the ear, it can be collected and sent to a laboratory to determine if any specific infectious organisms are present. Additionally, a tympanometry test will be performed. Here, the doctor inserts a probe into the ear which emits a tone with a certain amount of sound energy. The probe measures how much sound energy bounces back off the eardrum, rather than being transmitted to the middle ear. The more energy that is returned to the probe, the more blocked the middle ear is.
A diagnosis of acute otitis media is based on the following:
- recent, usually abrupt, onset of signs and symptoms of middle ear inflammation and middle ear effusion
- the presence of middle ear effusion that is indicated by any of the following: bulging of the tympanic membrane; limited or absent movement of the tympanic membrane; or discharge from the external ear
- signs or symptoms of middle ear inflammation as indicated by either distinct redness of the eardrum or ear pain that results in an interference with sleep or other normal activities
Otitis media with effusion can be more difficult to detect, since it is not painful and the child usually does not appear ill. The physician may rely on one or several tests to determine the diagnosis.
- A physical examination may reveal fluid behind the eardrum and poor movement of the eardrum. The eardrum may look clear and have no signs of redness, but may not move in response to air, as a normal eardrum would.
- A tympanometry test may reveal an impairment of eardrum mobility.
- A hearing test often shows some degree of hearing loss.
Treatment
Acute otitis media (AOM)
Treatment of AOM is focused on relieving any pain that may be present and addressing the infection itself. Usually, acetaminophen or ibuprofen prove adequate in
Occasionally, an "observation option" will be used in a child who has uncomplicated acute otitis media. This refers to delaying antibacterial treatment of certain children for 48 to 72 hours and limiting management to symptomatic relief. The decision to observe or treat is based on the child's age, the certainty of the diagnosis, and the severity of the illness. To observe a child without initial antibacterial therapy, it is important that the parent or caregiver has a ready means of communicating with the doctor. There also must be a system in place that permits a prompt reevaluation of the child if symptoms persist or worsen. If the decision is made to use an antibiotic, the usual recommendation is for amoxicillin, preferably at a dose of 80 to 90mg/kg/day. If the initial treatment plan fails to work within 48 to 72 hours, the physician may reconsider the diagnosis of AOM. Further treatment may involve changing antibiotics .
Otitis media with effusion (OME)
For young children ages one to three years, most physicians prefer a conservative, or wait-and-see, approach, using antibiotics if the infection is persistent, the child is in pain, or there is evidence of hearing loss. Most cases of otitis media with effusion get better within three months without any treatment. If the child continues to have repeated episodes of OME, despite taking antibiotics, the physician may decide to try long-term, low-dose treatment with antibiotics, even after the condition has cleared. If OME persists for over three months, despite antibiotic treatment, the doctor may suggest a hearing test. If OME persists for more than four to six months, even if hearing tests are normal, the doctor may suggest surgery to drain the eardrum and implant ear tubes for continuous drainage.
Surgery
In some cases, a surgical perforation to drain pus from the middle ear may be performed. This procedure is called a myringotomy . The hole created by the myringotomy generally heals itself in about a week. In 2002 a new minimally invasive procedure was introduced that uses a laser to perform the myringotomy. It can be performed in the doctor's office and heals more rapidly than the standard myringotomy. In some cases, the physician may decide that the placement of tubes during the myringotomy is recommended. These small tubes are placed to aid in draining the fluid from the middle ear. They fall out on their own after a few months. The decision to place these tubes is based on the following criteria:
- presence of fluid in the ears for more than three or four months following an ear infection
- fluid in the ears and more than three months of hearing loss
- changes in the structure of the eardrum as a result of ear infections
- a delay in speaking
- repeated infections that do not improve with antibiotics over several months
Another type of surgery, called an adenoidectomy, removes the adenoids. Removing the adenoids has been shown to help some children with otitis media between the ages of four to eight. It is a procedure generally reserved for those children who have recurrent otitis media after myringotomy tubes are extruded.
Alternative treatment
Treatment guidelines from the American Academy of Pediatrics and the American Academy of Family Physicians in the early 2000s state that there is insufficient evidence to either support or discourage the use of alternative medicines for acute otitis media. Increasing numbers of parents and caregivers are using various forms of nonconventional treatment for their children. Treatments that have been used for AOM include homeopathy, acupuncture, herbal remedies, chiropractic treatments, and nutritional supplements. Although most treatments are harmless, some are not. Some can have a direct and dangerous effect, whereas others may interfere with the effects of conventional treatments. Parent should inform their doctor if they are using any alternative or unconventional methods to treat their child's otitis media.
Prognosis
The prognosis of acute otitis media is excellent. The duration is variable. There may be improvement within 48 hours even without any treatment. Treatment with antibiotics for a week to 10 days is usually effective.
Prevention
Breastfeeding helps to pass along immunities to a child that may prevent otitis media. The position the child is in while breastfeeding is better than the usual bottle-feeding position for optimal eustachian tube function. If a child must be bottle-fed, it is best to hold the infant rather than allow him or her to lie down with the bottle. Because multiple upper respiratory infections may increase the risk for acute otitis media, reducing the exposure to large groups of children, particularly in daycare centers, may reduce the incidence. Children should also be kept away from environmental irritants such as secondhand tobacco smoke.
KEY TERMS
Adenoids —Common name for the pharyngeal tonsils, which are lymph masses in the wall of the air passageway (pharynx) just behind the nose.
Effusion —The escape of fluid from blood vessels or the lymphatic system and its collection in a cavity.
Eustachian tube —A thin tube between the middle ear and the pharnyx. Its purpose is to equalize pressure on either side of the ear drum.
Myringotomy —A surgical procedure in which an incision is made in the ear drum to allow fluid or pus to escape from the middle ear.
Nasopharynx —One of the three regions of the pharynx, the nasopharynx is the region behind the nasal cavity.
Ossicles —The three small bones of the middle ear: the malleus (hammer), the incus (anvil) and the stapes (stirrup). These bones help carry sound from the eardrum to the inner ear.
Parental concerns
A common concern among parents has been whether recurring episodes of otitis media will cause impairments in their child's development. Research indicates that persistent otitis media in the first three years of life does not have an adverse effect on development.
Resources
BOOKS
Friedman, Ellen M., et al. My Ear Hurts!: A Complete Guide to Understanding and Treating Your Child's Ear Infections. Collingdale, PA: DIANE Publishing Co., 2004.
Schmidt, Michael. A Parent's Guide to Childhood Ear Infection. Berkeley, CA: North Atlantic Books, 2004.
PERIODICALS
Huffman, Grace Brooke. "Should Recurrent Otitis Media Be Treated Surgically?" American Family Physician (February 15, 2000): 1128.
Kaye, Donald. "Primary Care Groups Issue Management Guidelines for Otitis Media." Clinical Infectious Diseases 38 (May 1, 2004): iv.
Rovers, Maroeska M., et al. "Otitis Media." The Lancet 363 (February 7, 2004): 465.
Wellbery, Caroline. "Effect of Otitis Media and Tympanostomy Tubes." American Family Physician 69 (March 1, 2004): 1237.
ORGANIZATIONS
American Academy of Otolaryngology—Head and Neck Surgery. One Prince Street, Alexandria, VA 22314. Web site: http://www.entnet.org.
American Academy of Pediatrics. 141 Northwest Point Boulevard, Elk Grove Village, IL 60007–1098. http://www.aap.org.
WEB SITES
"Chronic Otitis Media (Middle Ear Infection) and Hearing Loss." KidsENT. Available online at http://www.entnet.org/KidsENT/hearing_loss.cfm (accessed October 27, 2004).
"Ear Infections (Otitis Media)." Kidshealth. Available online at http://www.kidshealth.org/parent/infections/ear/otitis_media.html (accessed October 27, 2004).
Henderson, Sean O. "Pediatrics, Otitis Media." eMedicine. Available online at http://www.emedicine.com/emerg/topic393.htm (October 27, 2004).
Deanna M. Swartout-Corbeil, RN
Rosalyn Carson-DeWitt, MD
Rebecca J. Frey, PhD
I have a 2years old baby girl, she complained about her left ear pain and I put a small drop of olive oil and something came out like a worms inside and after she become OK after 2days she complained about the pain took her to a pharmacy they give her antibiotics powder and actamol syrup for pain to drink and after 2 days after taken the antibiotics the inner ear starts swollen she is crying about pain after 6 hours so please help. Can I take her to a doctor or wait for the antibiotics to get Finished.