Cochlear implants
Definition
A cochlear implant is a surgical treatment for hearing loss that works like an artificial human cochlea in the inner ear, helping to send sound from the ear to the brain. It is different from a hearing aid, which simply amplifies sound.
Purpose
A cochlear implant bypasses damaged hair cells in the child's cochlea and helps establish some degree of hearing by stimulating the hearing (auditory) nerve directly.
Description
Hearing loss is caused by a number of different problems that occur either in the auditory nerve or in parts of the middle or inner ear. The most common type of deafness is caused by damaged hair cells in the cochlea. The cochlea is a fluid-filled canal in the inner ear that is shaped like a snail shell. Inside are thousands of tiny hairs called cilia. As sound vibrates the fluid in the cochlea, the cilia move. This movement stimulates the auditory nerve and sends messages about sound to the brain. When these hair cells stop functioning, the auditory nerve is not stimulated, and the child cannot hear. Hair cells can be destroyed by many things, including infection, trauma, loud noise, aging, and birth defects.
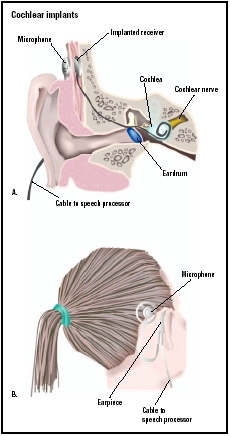
The first piece of a cochlear implant is the microphone. It is usually worn behind the ear, and it picks up sound and sends it along a wire to a speech processor. The speech processor is usually worn in a small shoulder pouch, pocket, or on a belt. The processor boosts the sound, filters out background noise, and turns the sound into digital signals. Then it sends these digital signals to a transmitter worn behind the ear. A magnet holds the transmitter in place through its attraction to the receiver-stimulator, a part of the device that is surgically attached beneath the skin in the skull. The receiver picks up digital information forwarded by the transmitter and converts it into electrical impulses. These electrical impulses flow through electrodes contained in a narrow, flexible tube that has been threaded into the cochlea during surgery and stimulate the auditory nerve. The auditory nerve carries the electrical impulses to the brain, which interprets them as sound.
Despite the benefits that the implant appears to offer, some hearing specialists and members of the deaf community still believe that the benefits may not outweigh the risks and limitations of the device. Because the device must be surgically implanted, it carries some surgical risk. Also, it is impossible to be certain how well any individual child will respond to the implant. After getting an implant, some people say they feel alienated from the deaf community, while at the same time not feeling fully a part of the hearing world.
The sounds heard through an implant are different from those sounds heard normally, and have been described as artificial or "robot-like." This is because the implant's limited number of electrodes cannot hope to match the complexity of a human's 15,000 hair cells. Cochlear implants are, however, becoming more advanced and providing even better sound resolution.
Surgical procedure
During the procedure, the surgeon makes an incision behind the ear and opens the mastoid bone (the ridge on the skull behind the ear) leading into the middle ear. The surgeon then places the receiver-stimulator into a well made in the bone and gently threads the electrodes into the cochlea. This operation takes between an hour-and-a-half and five hours. It is performed using general anesthesia.
Precautions
Because the implants are controversial, very expensive, and have uncertain results, the United States Food and Drug Administration (FDA) has limited the implants to people for whom the following is true:
- individuals who get no significant benefit from hearing aids
- individuals who are at least 12 months old
- individuals with severe to profound hearing loss
Preparation
Before a child gets an implant, specialists at an implant clinic conduct a careful evaluation, including extensive hearing tests to determine how well the child can hear.
First, candidates undergo a trial with a powerful hearing aid. If the hearing aid cannot improve hearing enough, a physician then performs a physical examination and orders a scan of the inner ear, because some patients with a scarred cochlea are not good candidates for cochlear implants. A doctor may also order a psychological exam to better understand the person's expectations. Patients and their families need to be highly motivated and have a realistic understanding of what an implant can and cannot do.
Aftercare
The child may remain in the hospital for a day or two after the surgery, although with improving technology and techniques some children may go home the same day. After about a month, the surgical wounds will have healed, and the child returns to the implant clinic to be fitted with the external parts of the device (the speech processor, microphone, and transmitter). A clinician tunes the speech processor and sets levels of stimulation for each electrode from soft to loud.
The child is then trained in how to interpret the sounds heard through the device. The length of the training varies from days to years, depending on how well the child can interpret the sounds heard. With the new approval for using cochlear implants in children as young as 12 months of age, the toddler may not be trained specifically to interpret the sounds in the same way an older child would. The specific therapy that is recommended is highly dependent on the age of the child.
Risks
As with all operations, there are a few risks of surgery. These include the following:
- dizziness
- facial paralysis (which is rare and usually temporary)
- infection at the incision site
Scientists are not sure about the long-term effects of electrical stimulation on the nervous system. It is also possible that the implant's internal components may be damaged by a blow to the head. This may cause the device to stop working. In general the failure rate of the implants is only 1 percent after one year.
Parental concerns
There is increasing debate about the use of cochlear implants in infants. This is considered by some to be desirable because, if the implantation is done before a child has begun to significantly acquire language, there is some evidence that the child may be able to develop at a pace similar to hearing children of the same age. Making a decision about whether or not a child, especially a very young one, should have a cochlear implant can be very difficult. The child's doctor may be able to provide parents with resources or put them in contact with other parents who have had to make the same decision whom they can consult.
KEY TERMS
Cochlea —The hearing part of the inner ear. This snail-shaped structure contains fluid and thousands of microscopic hair cells tuned to various frequencies, in addition to the organ of Corti (the receptor for hearing).
Hair cells —Sensory receptors in the inner ear that transform sound vibrations into messages that travel to the brain.
Inner ear —The interior section of the ear, where sound vibrations and information about balance are translated into nerve impulses.
Middle ear —The cavity or space between the eardrum and the inner ear. It includes the eardrum, the three little bones (hammer, anvil, and stirrup) that transmit sound to the inner ear, and the eustachian tube, which connects the inner ear to the nasopharynx (the back of the nose).
See also Hearing impairment .
Resources
BOOKS
Christiansen, John B., and Irene W. Leigh. Cochlear Implants in Children: Ethics and Choices. Washington DC: Gallaudet University Press, 2002.
Chute, Patrician M., and Mary Ellen Nevins. The Parents' Guide to Cochlear Implants. Washington DC: Gallaudet University Press. 2002.
PERIODICALS
Barker, Brittan A., and Bruce J. Tomblin. "Bimodal Speech Perception in Infant Hearing Aid and Cochlear Implant Users." Archives of Otolaryngology—Head & Neck Surgery 130 (May 2004): 582–87.
Chin, Steven B. "Children's Consonant Inventories after Extended Cochlear Implant Use." Journal of Speech, Language, and Hearing Research 46 (August 2003): 849–63.
Conor, Carol McDonald, and Teresa A. Zwolan. "Examining Multiple Sources of Influence on the Reading Comprehension Skills of Children Who Use Cochlear Implants." Journal of Speech, Language, and Hearing Research 47 (June 2004): 509–27.
ORGANIZATIONS
American Society for Deaf Children. PO Box 3355 Gettysburg, PA 17325. Web site: http://www.deafchildren.org.
Tish Davidson, A.M. Carol A. Turkington