Patent ductus arteriosus
Definition
Patent ductus arteriosus (PDA) is a heart defect that occurs in infants when the ductus arteriosus (the temporary fetal blood vessel that connects the aorta and the pulmonary artery) does not close at birth.
Description
The ductus arteriosus is a temporary fetal blood vessel that connects the aorta and the pulmonary artery before birth. The ductus arteriosus should be present and open before birth while the fetus is developing in the uterus. Since oxygen and nutrients are received from the placenta and the umbilical cord instead of the lungs, the ductus arteriosus acts as a "short cut" that allows blood to bypass the deflated lungs and go straight out to the body. After birth, when the lungs are needed to add oxygen to the blood, the ductus arteriosus normally closes. The closure of the ductus arteriosus ensures that blood goes to the lungs to pick up oxygen before going out to the body. Closure of the ductus arteriosus usually occurs at birth as levels of certain chemicals, called prostagladins, change, and the lungs fill with air. If the ductus arteriosus closes correctly, the blood pumped from the heart goes to the lungs, back into the heart, and then out to the body through the aorta. The blood returning from the lungs and moving out of the aorta carries oxygen to the cells of the body. In some infants, the ductus arteriosus remains open (or patent), and the resulting heart defect is known as patent ductus arteriosus. In most cases, a small PDA does not result in physical symptoms. If the PDA is larger, health complications may occur.
In an average individual's body, the power of blood being pumped by the heart and other forces leads to a certain level of pressure between the heart and lungs. The pressure between the heart and lungs of an individual affected by PDA causes some of the oxygenated blood that should go out to the body (through the aorta) to return back through the PDA into the pulmonary artery. The pulmonary artery takes the blood immediately back to the lungs. The recycling of the already oxygenated blood forces the heart to work harder as it tries to supply enough oxygenated blood to the body. In this case, usually the left side of the heart grows larger as it works harder and must contain all of the extra blood moving back into the heart. This is known as a left-to-right or aortic-pulmonary shunt.
As noted, the size of the PDA determines how much harder the heart has to work and how much bigger the heart becomes. If the PDA is large, the bottom left side of the heart is forced to pump twice as much blood because it must supply enough blood to recycle back to the lungs and move out to the body. As the heart responds to the increased demands for more oxygenated blood by pumping harder, the pulmonary artery has to change in size and shape in order to adapt to the increased amount and force of the blood. In some cases, the increase in size and shape changes the pressure in the pulmonary artery and lungs. If the pressure in the lungs is higher than that of the heart and body, blood returning to the heart will take the short cut back into the aorta from the pulmonary artery through the PDA instead of going to the lungs. This backward flowing of blood does not carry much oxygen. If blood without much oxygen is being delivered to the body, the legs and toes will turn blue or cyanotic. This condition is called a shunt reversal.
When a PDA results in a large amount of blood being cycled in the wrong order, either through a left-to-right shunt or shunt reversal, the overworked, enlarged heart may stop working (congestive heart failure) and the lungs can become filled with too much fluid (pulmonary edema). At this time, there is also an increased risk for bacterial infection that can inflame the lining of the heart (endocarditis). These three complications are very serious.
Demographics
PDA is a very common heart defect, accounting for 5 to 10 percent of all types of congenital heart disease . Though an exact incidence of PDA is difficult to determine, researchers estimate that eight or nine in every 1,000 children are affected. PDA can occur in full-term infants, but it is seen most often in preterm infants, infants born at a high altitude, and babies whose mothers had a rubella infection during pregnancy. PDA occurs in individuals of every ethnic origin and does not occur more often in any one country or ethnic population; however, it is two to three times more common in females than males.
Causes and symptoms
PDA can be caused by environmental exposure before birth or the inheritance of a specific changed or mutated gene or genes. It can be a symptom of a genetic syndrome or may be caused by a combination of genetic and environmental factors (multifactorial).
Environmental exposures that can increase the chance for a baby to be affected by PDA include fetal exposure to rubella before birth, preterm delivery, and birth at a high altitude location.
PDA can be an inherited condition in families with isolated PDA or part of a genetic syndrome. In either case, there are specific gene changes or mutations which lead to a defect in the elastic tissue forming the walls of the ductus arteriosus. As of 2004 the genes causing isolated PDA have not been identified, but it is known that PDA can be inherited through a family in an autosomal dominant pattern or an autosomal recessive pattern. Every person has approximately 30,000 genes, which tell the body how to grow and develop correctly. Each gene is present in pairs since one is inherited from the mother and one is inherited from the father. In an autosomal dominant condition, only one specific changed or mutated copy of the gene for PDA is necessary for a person to have PDA. If a parent has an autosomal dominant form of PDA, there is a 50 percent chance for each child to have the same or similar condition.
PDA can also be inherited in an autosomal recessive manner. A recessive condition occurs when a child receives two changed or mutated copies of the gene for a particular condition, such as PDA (one copy from each parent). Individuals with a single changed or mutated copy of a gene for a recessive condition are known as carriers and have no health problems related to the condition. However, when two people who each carry a changed or mutated copy of the same gene for a recessive condition have children, there is a chance with each pregnancy for the child to inherit the two changed or mutated copies from each parent. In this case, the child would have PDA. For two known carriers, there is a 25 percent risk with each child to have a child with PDA, a 50 percent chance to have a child who is a carrier, and a 25 percent chance to have a child who is neither affected nor a carrier.
Most cases of PDA occur as the result of multifactorial inheritance which is caused by the combination of genetic factors and environmental factors. The combined factors lead to isolated defects in the elastic tissue forming the walls of the ductus arteriosus.
The main sign of PDA is a constant heart murmur that sounds like the hum of a refrigerator or other machinery. This murmur is usually heard by the doctor using a stethoscope.
Other signs and symptoms of PDA include:
- shortness of breath after exertion such as crying, eating, or activity
-
labored or fast breathing at rest
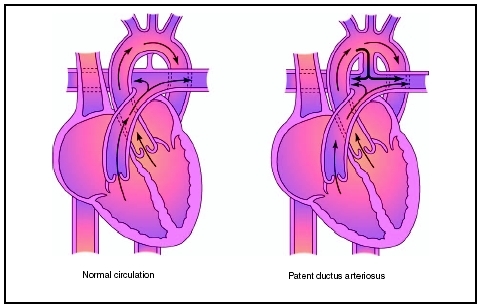 Patent ductus arteriosus (PDA) is the failure of the ductus arteriosus to close after birth, allowing blood to inappropriately flow from the aorta into the pulmonary artery.(Illustration by Electronic Illustrators Group.)
Patent ductus arteriosus (PDA) is the failure of the ductus arteriosus to close after birth, allowing blood to inappropriately flow from the aorta into the pulmonary artery.(Illustration by Electronic Illustrators Group.) - cyanosis, or blue lips or fingernails especially after eating, crying, or activity
- problems with feeding and poor weight gain
- frequent colds and problems with the lungs
Diagnosis
Diagnosis is most often made by detecting the characteristic "machinery" heart murmur heard by a doctor through a stethoscope. Tests such as a chest x ray, echocardiograph, and ECG are used to support the initial diagnosis and to determine the severity of the PDA.
Treatment
The treatment and management of PDA depends upon the size of the PDA, the presence of other heart defects, and the symptoms experienced by the affected individual. In some cases, the PDA will close spontaneously and no further treatment will be required. In individuals for whom the PDA remains open, there are three treatment options: medical management, device closure, and surgical repair.
Medical management with medications such as indomethocin is often the first course of treatment in premature infants with PDA. Indomethocin causes the muscles within the heart to tighten, closing the PDA. In infants for whom indomethocin does not close the PDA, full-term infants, and older children, device closure or surgery may be necessary.
Device closure of PDA is a medical procedure in which a device such as a coil, very small rings of wire, or an occluder, a tiny wire mesh patch, is placed over the PDA causing the blood to clot and thus closing the open ductus. The device is inserted into the heart in a process called cardiac catheterization. A small thin flexible tube is inserted into a blood vessel, usually in the groin area, and guided into the heart. The device is then passed through the catheter to the PDA. For most patients, this procedure is highly effective, and no further treatment is required. In children for whom this procedure is unsuccessful, children with very large PDA, or those with multiple heart defects, surgery may be necessary.
In surgical closure of PDA, called a ligation, the chest cavity is opened, the blood vessels are separated, and the PDA is sewn closed.
Prognosis
Individuals can survive with a small opening remaining in the ductus arteriosus. Treatment, including surgery, of a larger PDA is usually successful and frequently occurs without complications. Proper treatment allows children to lead normal lives.
Prevention
While there is no known prevention for PDA, appropriate prenatal care for expectant women is important and may prevent premature delivery, a major risk factor for PDA.
Parental concerns
Slow weight gain is common in children with congenital heart defects and may be alarming for parents. The pediatrician closely monitors the child's growth rate. There are many ways to increase the caloric intake of infants and children with PDA. A pediatrician, nurse, or dietitian can assist parents in ways to insure the child is getting proper nutrition . Infants with PDA may not be able to tolerate a large volume of breast milk or formula and therefore may need to be fed more frequently.
KEY TERMS
Aorta —The main artery located above the heart that pumps oxygenated blood out into the body. The aorta is the largest artery in the body.
Cyanosis —A bluish tinge to the skin that can occur when the blood oxygen level drops too low.
Ductus arteriosus —The temporary channel or blood vessel between the aorta and pulmonary artery in the fetus.
Echocardiogram —A record of the internal structures of the heart obtained from beams of ultrasonic waves directed through the wall of the chest.
Electrocardiagram (ECG, EKG) —A record of the electrical activity of the heart, with each wave being labeled as P, Q, R, S, and T waves. It is often used in the diagnosis of cases of abnormal cardiac rhythm and myocardial damage.
Endocarditis —Inflammation of the inner membrane lining heart and/or of the heart valves caused by infection.
Oxygenated blood —Blood carrying oxygen through the body.
Pulmonary artery —An artery that carries blood from the heart to the lungs.
Pulmonary edema —An accumulation of fluid in the tissue of the lungs.
In addition to slow growth, children with PDA may be more susceptible to infections such as colds, pneumonia , and a rare but potentially life threatening infection of the heart called endocarditis. Children with PDA may need to receive preventative antibiotics prior to dental work. Annual flu vaccines are recommended, and parents should watch for signs of infection such as fever , cough , chills, and any difficulty breathing.
When to call the doctor
Parents of children with PDA should watch for the following symptoms and contact the doctor if any of these occurs:
- problems feeding or slow weight gain
- difficulty breathing
- shortness of breath after crying, eating, or activity
- blue color in the lips and fingernails with activity
- fever of 100.4°F (38°C) or higher
- chills, cough, or lethargy
- itchy rash or swollen skin
Resources
ORGANIZATIONS
Congenital Heart Anomalies Support, Education, and Resources (CHASER). 2112 North Wilkins Rd., Swanton, OH 43558. Web site: http://www.csun.edu/~hfmth006/chaser.
Kids with Heart. 1578 Careful Dr., Green Bay, WI 54304. Web site: http://www.execpc.com/~kdswhrt.
WEB SITES
"Patent Ductus Arteriosus: Signs, Symptoms, Diagnosis, Treatment, Benefit." Heart Center Encyclopedia, Cincinnati Children's Hospital Medical Center. Available online at http://www.cincinnatichildrens.org/health/heartencyclopedia/anomalies/pda.htm.
Pflieger, Kurt. "Patent Ductus Arteriosus." emedicine , October 29, 2002. Available online at http://www.emedicine.com/emerg/topic358.htm.
Dawn A. Jacob Deborah L. Nurmi, MS
Comment about this article, ask questions, or add new information about this topic: