Myopia
Definition
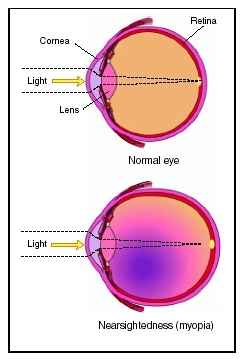
Myopia, or nearsightedness, is a condition in which objects in the distance are blurred either because the eye is too long or too strong. It is the result of both environmental and genetic factors.
Description
The degree to which one is myopic depends on the powers of the cornea and the lens of the eye and the length of the eyeball. In a normal eye the incoming visual images meet on the retina in the back of the eye. If these visual images converge in front of the retina instead of on the retina, then one is myopic.
There are several types of myopia, of which simple myopia is the most common. Individuals with simple myopia have eyes that are either too long or too powerful. Congenital myopia develops in infants. Individuals with high myopia, greater than six diopters, can develop pathological changes in the retina, called degenerative myopia. Nocturnal myopia, another type of myopia sometimes referred to as "night blindness," is blurred vision only in darkness. Myopia can also be induced by co-existing medical problems and drug exposure.
A child's refractive status or power of the eye when he or she begins school is a good indicator of whether the child will become nearsighted. Most children are hyperopic, or far-sighted, at birth and experience a decrease in far-sightedness throughout early childhood. Myopia is less likely to develop by age 13 if a child still has at least 0.75 diopters of hyperopia at age eight. But if a child has become at least 0.25 diopters myopic at this age then there is a 60 percent chance that the child will require spectacle correction for nearsightedness by age 13.
Myopia does decreases in later life. This appears not to be related to a decrease in close work as is often suggested but rather due to some factor intrinsically related to ageing. It has been hypothesized the power of the lens of the eye changes in later life.
High myopia has been associated with various syndromes: Ehlers-Danlos, Marfan, Down, and Stickler syndromes. Myopia is often observed in retinopathy of prematurity (ROP). ROP is seen in 68 percent of infants with low birth weights and over 80 percent of infants born with ROP will be myopic. The myopia associated with ROP increases through age five, after which it stabilizes.
Transmission
Although no gene for myopia has been isolated, heredity is believed to play a role in myopia. If both parents are myopic, then the odds that the child will be myopic are as high as 60 percent. This drops to at most 40 percent when only one parent is nearsighted, and for 15 percent of myopic children, neither parent has myopia. High myopia is especially likely to have a genetic component.
Demographics
Overall, 25 percent of those living in the United States are myopic. Myopia is slightly more prevalent among females than males, and among those with advanced academic training. Less than 5 percent of five year olds are myopic, but this percentage increases to 25 percent by late teens and to approximately 35 percent for young adults and to 42 percent of those middle-aged. These percentages decrease to 20 percent by age 65 and to less than 13 percent by age 80.
Myopia is more prevalent in Asian countries; as much as 70 percent of the Chinese population is nearsighted.
Causes and symptoms
Congenital myopia develops because of an obstruction along the visual pathway such as cataract. The eye becomes elongated in response to blur these causes, creating a myopic eye.
A first sign that a child might have myopia is difficulty in seeing things in the distance, such as the chalkboard. The child may not see things in the distance as well as a classmate or sibling.
For the 2 percent of the population who are extremely nearsighted, an inherently weak sclera, whose fibers are not held together tightly, causes the eye to stretch. This stretching can continue into adulthood, increasing myopia.
Other causes of increasing nearsightedness include difficulty with converging, the process through which the eyes move inwardly together when reading, and esophoria, the condition in which the eyes are more comfortable positioned close to the nose. Doing a lot of close work, such as playing video games and using the computer for extended periods, may increase myopia for these children.
Causes of induced myopia include cataracts and elevations of blood sugar in diagnosed or undiagnosed diabetics. Some drugs, such as corticosteroids, antihistamines , and some antibiotics , including sulfonamides , can induce myopia.
Another cause of increasing myopia is the over wearing of contact lenses . Swelling of the cornea can occur if the eye does not have sufficient oxygen causing a transient increase in myopia. Silicone contact lenses allow a marked increase in oxygen to reach the eye decreasing the probability of myopic increases.
For the child with diabetes, fluctuations in blood sugars can cause swelling of the cornea of the eye, leading to transient increases in myopia, which stabilize once the diabetes is controlled. But the child may independently become more myopic later in life.
In the early 2000s, it has been suggested that insulin resistance, which accompanies type 2 diabetes and prediabetes, may increase myopia in children and adolescents. The level of insulin-like growth factor binding protein 3 (IGFBP-3), a hormone that works with insulin to lower blood glucose levels, is low in individuals who are insulin resistant. This decreased level, in turn, decreases the sensitivity of ocular tissue to another compound called retinoic acid, which prevents increases in the length of the eye. Thus, if insulin levels are higher than normal, the risk of myopia may be increased.
Asthenopia or a feeling of eye strain is not common in myopia. If a child complains of eye strain, then usually there is another cause of the eye strain, including an astigmatism, a condition in which the eye is football shaped; anisometropia, a condition in which the eyes are of different powers; or difficulty with focusing.
When to call the doctor
There are many reasons why a child cannot see well in the distance. Myopia is the most common cause of distance blur, and since much of what a child learns comes from vision and visual cues, correction of myopia is important. Also, problems with vision may be a sign of a more serious ocular problem, such as cataracts, or of a medical problem, such as diabetes.
Diagnosis
Myopia is diagnosed by determining a child's unaided vision and is confirmed objectively by the eye care practitioner with various techniques, including retinoscopy and refraction.
The type and extent of myopia is determined by additional testing. These tests include an evaluation of the child's binocular vision, his eye movements, his ability to converge and focus on objects close-up, and his ocular health. Dilation of the eye allows the doctor to check for complications of ROP, diabetes, or degenerative myopia. Since children are capable of over focusing, dilation can help the eye care practitioner determine a child's true prescription because the drugs used to dilate also impair this tendency to over focus. Over focusing can cause a child to appear to be myopic when he or she is actually not.
Treatment
Myopia is most commonly treated with spectacles or glasses. Myopia in preschool children does not need to be corrected with glasses, unless either anisometropia, a condition in which there is a difference of more than 1.00 diopters between the two eyes, or amblyopia , a condition in which a child cannot be corrected to 20/20 with spectacles, is present. As the child enters school, distance vision becomes critical for learning, and children with prescriptions of at least 1.00 diopter of myopia or who have 20/40 vision or worse should be given glasses. Once a child is diagnosed with myopia, he or she should be examined every six months to a year, and each eye should be corrected to 20/20 at each visit. The glasses are then usually worn full time, except for children with difficulty with convergence (esophoria), who may remove their glasses for close work.
Some adolescents may want to wear contact lenses. Wearing contact lenses can improve appearance. Peripheral vision is improved with contact lenses, especially for those with high degrees of myopia or who have anisometropia.
Rigid gas permeable (RGPs) contact lenses are used to correct myopia. The rate at which myopia increases may be slowed by RGP lenses. RGPs are also employed in orthokeratology, a technique in which RGP lenses of gradually decreasing flatness are worn for specified amounts of time. These lenses, called ortho-K lenses, flatten the cornea, changing the power of the cornea over time and decreasing myopia. This effect of ortho-K lenses is not permanent and an ortho-K lens must be worn periodically or the original myopia reappears. For some individuals—for example, those with keratoconnus, a disease of the cornea—RGPs may offer the only way to correct vision.
For some children the development of myopia may be slowed with reading glasses or bifocals. If bifocals are prescribed, then either progressive or no-lines, or a lined bifocal may be given. If a lined bifocal is prescribed, then the line is always placed higher for the child than for the adult. This is done to encourage use of the power of the bifocal.
Refractive surgery is also used to correct myopia, but only on fully grown individuals. A child's eyes change and the safety of these procedures have not been established in the growing eye.
The most common surgical procedure performed to correct myopia is laser in situ keratomileusis (LASIK). Other techniques to correct myopia include photorefractive keratectomy (PRK), radial keratomy (RK), laser epithelial keratomileusis (LASEK), intraocular lens
Alternative treatment
Cycloplegic drugs, such as atropine, may decrease myopia, but they may hinder the child's ability to see up close. As of 2004 pirenzepine, which has shown to decrease the rate of myopia in children without sacrificing the ability of the child to do close work, is in clinical trial.
Prognosis
Most infants are born far-sighted and eventually reach emmetropia or normal vision, by age six. Over one third of children go on to become myopic as adults.
Patients with high myopia, greater than 6.00 diopters, have an increased risk of developing a retinal tear, hole, or detachment; a posterior staphyloma; a posterior vitreous detachment; or glaucoma. Rarely are these pathological changes of myopia seen in children or adolescents. Retinal detachments and tears are possible, however, in highly myopic children or adolescents who play contact sports . If a retinal problem is diagnosed or suspected, referral to a retinal specialist is necessary.
Prevention
For individuals who have difficulty with convergence or focusing or who are esophoric, close work may increase myopia. Children diagnosed with these problems would benefit from frequent breaks while doing close work. Increases in myopia for these children may be slowed with bifocals and/or removal of glasses for reading and homework.
Nutritional concerns
Since elevated levels of insulin may be associated with increased myopia; a diet low in those foods that increase insulin secretion, such as refined carbohydrates, may help decrease myopia.
Parental concerns
Children rely on their vision in their learning processes; if they have difficulty seeing this handicap affects academic performance. Thus, any vision problem should be corrected promptly. Once myopia is diagnosed, it typically increases through childhood and vision correction is needed for classroom work and for sports. If a child is not corrected fully and continues to have blurred vision, the eye may elongate in response to blur, perpetuating the myopia.
Myopia cannot be diagnosed by school screenings or by simply reading eye chart at the pediatrician's office. A comprehensive eye exam as given by an ophthalmologist or an optometrist is needed, if myopia is suspected. Most cases of myopia result from changes within the eye, but the condition can be a manifestation of other more serious problems, such as cataract or diabetes.
KEY TERMS
Accommodation —The ability of the lens to change its focus from distant to near objects and vice versa. It is achieved through the action of the ciliary muscles that change the shape of the lens.
Anisometropia —An eye condition in which there is an inequality of vision between the two eyes. There may be unequal amounts of nearsightedness, farsightedness, or astigmatism, so that one eye will be in focus while the other will not.
Astigmatism —An eye condition in which the cornea doesn't focus light properly on the retina, resulting in a blurred image.
Cataract —A condition in which the lens of the eye turns cloudy and interferes with vision.
Convergence —The natural movement of the eyes inward to view objects close-up.
Cornea —The clear, dome-shaped outer covering of the eye that lies in front of the iris and pupil. The cornea lets light into the eye.
Diopter (D) —A unit of measure for describing the refractive power of a lens.
Emmetropia —Normal vision.
Retina —The inner, light-sensitive layer of the eye containing rods and cones. The retina transforms the image it receives into electrical signals that are sent to the brain via the optic nerve.
Sclera —The tough, fibrous, white outer protective covering of the eyeball.
See also Diabetes mellitus ; Ehlers-Danlos syndrome ; Marfan's syndrome .
Resources
BOOKS
Cordain, Loren. The Paleo Diet. Hoboken, NJ: John Wiley & Sons, 2002.
Murillo-Lopez, Fernando H. "Myopia." In Current Ocular Therapy. Philadelphia: Saunders, 2000.
Prett, Ronald C. "Pathologic Myopia." In Principles and Practice of Ophthalmology. Philadelphia: Saunders, 2000.
Steidl, Scott M., and Ronald C. Pruett. "Myopia and Systemic Disorders." In Principles and Practice of Ophthalmology. Philadelphia: Saunders, 2000.
PERIODICALS
Byrne, Jennifer. "Pirenzepine Showing Promise in Clinical Trials for Topical Myopia Treatment." Primary Care Optometry News 8, no. 10 (October 2003): 10–1.
Cordain, Loren, et al. "An Evolutionary Analysis of the Aetiology and Pathogenesis of Juvenile-Onset Myopia." Acta Ophthalmologica Scandinavica 80, no. 2 (April 2002): 125–35.
Karpecki, Paul M. "What's New in Refractive Surgery." Review of Optometry (May 15, 2001): 71–4.
Karpecki, Paul M., and Marc Bloomenstein. "Phakic IOLs: The LASIK Alternative." Review of Optometry (February 15, 2003): 91–2.
Mutti, Donald O., and Karla Zadnik. "Age-Related Decreases in the Prevalence of Myopia: Longitudinal Change of Cohort Effect?" Investigative Ophthalmology & Visual Science 41, no. 8 (July 2000): 2103–07.
WEB SITES
"Myopia (Nearsightedness)." All About Vision. Available online at http://www.allaboutvision.com/conditions/myopia.htm (accessed November 30, 2004).
Martha Reilly, OD