Dental development

Definition
Dental development is the process by which children develop their first and second (permanent) teeth.
Description
A child's first set of 20 teeth are called baby, primary, deciduous, or milk teeth. As these teeth fall out, they are replaced by 32 permanent, adult, or secondary teeth. The entire process of dental development may take more than two decades. Both primary and permanent teeth usually erupt (break through the gum) in a specific order on each side of the upper and lower jaws. However, the timing of both primary and permanent tooth eruption can vary by two or more years.
Both the timing of dental development and tooth size are determined primarily by heredity. Individuals differ greatly in the size of the crown (the part of the tooth above the gum line). Except for the earliest stages of prenatal development , and possibly the third permanent molars or wisdom teeth, dental development in girls proceeds ahead of that in boys, often by as much as 6 percent. Girls also have slightly smaller crowns and slightly shorter tooth roots than boys.
Prenatal
Dental development begins at about three weeks of gestation. By six weeks of gestation the tips or cusps of the primary teeth appear. By the fourth month the hard tissues (the enamel and dentin) of the primary teeth have begun to form. The enamel crowns of most primary teeth are fully formed by eight months of gestation. Permanent teeth begin to form shortly before or at birth.
Baby teeth
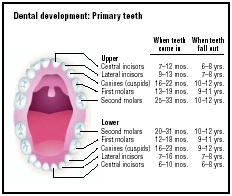
At birth the developing teeth usually are still embedded in the gums. Occasionally a baby is born with some erupted teeth or teeth that erupt shortly after birth. These natal or neonatal teeth usually are poorly formed and mobile. However in most infants the front teeth begin to peek through the gums between four and eight months. Generally from about six months on, children get four new teeth every four months. By 12 to 15 months all of the baby teeth within the gums have formed crowns. Most children have all 20 baby teeth by the age of two-and-a-half to three years. The permanent teeth continue to develop within the jaw.
Baby teeth erupt in pairs on the right and left of the mouth, alternating between the lower and upper jaws, and proceeding from front to back. The 20 primary teeth usually erupt in the following order:
- four front teeth or central incisors, first in the lower jaw and then in the upper jaw
- four lateral incisors, on each side of the front teeth, uppers before lowers
- four first molars, uppers first
- four canines or cuspids, between the lateral incisors and the first molars, usually uppers before lowers
- four second molars behind the first molars, lowers first
Baby teeth may come in straight or at an angle, appearing crooked, although they eventually straighten out. Once all of the baby teeth have erupted, the tongue adapts to their shape and the child's pre-teeth swallowing pattern switches to an adult pattern.
Children start losing their baby teeth at about age six, after the permanent front teeth are almost formed beneath the gums. The pressure of the developing permanent teeth causes the roots of the baby teeth to dissolve. Without their anchor in the jaw, the baby teeth loosen and eventually fall out. Most children lose their lower front baby teeth first. The earlier that the baby teeth come in, the earlier they will fall out. Most children have lost all of their baby teeth by age 13.
Permanent teeth
Between the ages of two-and-a-half and six, the permanent teeth continue to develop within the jaw. The first permanent teeth, the six-year-molars that become the first permanent molars, erupt behind each of the four second baby molars, usually between the ages of five and six. If the baby teeth are properly positioned and aligned, the six-year-molars usually erupt properly. If the baby teeth are pushed too close together, the six-year-molars will be too far forward, crowding the permanent teeth that erupt in front of them. However if the six-year-molars erupt properly and if the jaw is large enough, the permanent teeth have a good chance of coming in correctly.
By about age eight, enamel has formed on all of the permanent teeth except the wisdom teeth. A permanent tooth comes in completely about two months after the corresponding baby tooth is lost. Between the ages of about six and 12 to 14, as the jaw grows, 28 permanent teeth erupt, replacing the primary teeth, incisor for incisor, canine for canine, premolar or bicuspid for molar. The 32 permanent teeth generally erupt in the following order:
- four six-year or first molars
- four central incisors or front teeth, first in the lower jaw and then in the upper jaw
- four lateral incisors, lowers usually first
- four canine teeth, lowers first
- four first premolars or bicuspids, between the canines and the six-year molars, uppers usually first
- four second premolars or bicuspids, between the first premolars and the six-year or first molars, uppers usually first
- four second molars, behind the first molars, lowers usually first
- four third molars or wisdom teeth at the back, usually between ages 17 and 21
Common problems
Teething
Teething (the eruption of the primary teeth through the gums) may cause discomfort or pain , particularly with the large molars. Teething babies may:
- be restless and irritable
- lose their appetites
- sleep poorly
- cry excessively
- have flushed cheeks
- have a slight fever
- have congestion
- dribble or drool
- have red, swollen gums at the new teeth sites
- rub their gums
- suck their thumbs
- want something to chew on
For teething symptoms, parents may massage the gums to relieve discomfort and offer teething toys to help speed tooth eruption. A frozen teething toy numbs the gums and reduces swelling, although it should not be left on the gum for more than one minute without a break. They may also relieve symptoms by the following:
- massaging the gums, with or without ice
- giving the baby a cold teething ring
- encouraging the baby to chew on cold, wet washcloth or frozen bagel
- administering acetaminophen (Tylenol)
Eruptions of the permanent teeth are usually much less distressing, although the eruption of the first four broad permanent molars may cause discomfort. As the permanent molars push through the gums, they often leave a flap of tissue over the tooth. If food becomes trapped under the flap, the gums may become sore, swollen, and painful, infected, or abscessed.
Developmental delay
While dental development may be slightly advanced in obese children, development delay can occur with the emergence of some permanent teeth. Delay can be caused by the following:
- hereditary factors
- chronic malnutrition
- developmental disorders
- hyperdontia (extra or supernumerary teeth)
- Down syndrome
- radiation or chemotherapy
- cysts or tumors
- the absence of lateral incisors or wisdom teeth
Decay
The enamel on baby teeth is thinner and softer than on permanent teeth and decay can move through it very rapidly. Some children develop decay as soon as a tooth erupts and about 50 percent of two-year-olds have at least one cavity.
Baby bottle tooth decay occurs when sugary liquids, including milk, juice, or formula, cling to the baby's teeth, particularly when the child is put to bed with a bottle. The decay occurs most often in the upper front teeth but other teeth also can be affected. If a decayed baby tooth is lost too early, the adjacent teeth may move into the space, causing crooked and overcrowded permanent teeth.
Malocclusion
In a perfect jaw, all of the teeth fit exactly without crowding or spacing. The teeth are not rotated, twisted, or leaning forward or backward. With a perfect bite (occlusion), the teeth of the upper jaw slightly overlap those of the lower jaw. The points of the molars fit into the grooves of the opposing molars.
Few children develop perfect teeth and occlusion. More than 90 percent of children have some degree of malocclusion or poor bite. Skeletal malocclusions occur when the upper and lower jaws are not properly aligned with each other and with the skull. Dental malocclusions occur when the teeth are crowded or the upper and lower teeth are not properly aligned with each other. Malocclusions can be caused by the following:
- heredity
- crowded or misaligned baby teeth
- premature loss of baby teeth due to decay or injury, so that the permanent first molars move forward, causing crowding and misalignment of the new front teeth
- loss of permanent tooth structure due to untreated decay in the baby teeth
- a tooth emerging at an angle such that it pushes on and damages an adjacent tooth
- sucking that continues after the permanent teeth erupt
- wisdom teeth that erupt crookedly
- accidental injury
Some children experience mild, temporary symptoms of malocclusion resulting from a growth spurt. Severe malocclusion may require orthodontic intervention to improve appearance or to prevent problems with eating and speaking. Most alignment problems develop gradually, although they may be apparent at eruption. Symptoms of alignment problems include the following:
- lack of space between teeth
- teeth that are out-of-line or abnormally spaced
- front teeth that do not meet
- protruding of the upper or lower jaw
- protruding upper front teeth (overbite)
- protruding lower front teeth (underbite)
- an open bite wherein the upper and lower front teeth do not touch during biting
Developmental disorders
Dental development disorders may occur as a result of the following:
- numerous inherited syndromes
- improper prenatal development
- endocrine disorders
- environmental factors
Developmental disorders include the following:
- hypodontia, in which one or more permanent teeth, usually the wisdom teeth or the lateral incisors, fail to form and the remaining teeth tend to be smaller
- anodontia, a very rare condition in which many or all of the permanent teeth fail to form
- supernumerary or extra teeth (These are more common in permanent teeth than in baby teeth; extra teeth usually are somewhat shapeless pegs, although occasionally an extra molar develops fully.)
Discolored and misshapen teeth
Disorders that may cause discoloration of the teeth include:
- hypoplasia, in which insufficient or irregular enameling of the teeth caused by the administration of tetracycline to a pregnant or nursing mother or to the infant or young child
-
enamel and dentin hypoplasia, in which the enamel and dentin are not
calcified (hardened by the depositing of
minerals
) due to
vitamin D deficiency
during tooth development
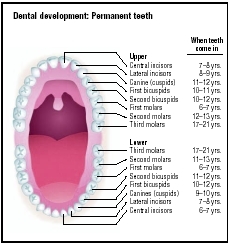 Illustration of the eruption of permanent teeth.(Illustration by GGS Information Services.)
Illustration of the eruption of permanent teeth.(Illustration by GGS Information Services.) - hypocalcification, in which the enamel is of poor quality due to genetic factors, extensive plaque deposits, excessive sucking on citrus fruits, or high consumption of very acidic carbonated beverages
- amelogenesis imperfecta, an inherited defect that causes thin and discolored enamel
- dentinogenesis imperfecta, a defect of the dentin that causes discoloration and loss of enamel
- extrinsic enamel coloration due to liquid iron supplements administered for anemia or due to plaque or stains adhering to calculus, hard mineral deposits on the crowns and roots
- intrinsic enamel coloration due to pigments carried in the blood from tetracycline or other drugs or from excessive fluoride
Illness or trauma during infancy or early childhood, including infections, high fever, malnutrition, or disorders such as congenital syphilis or Down syndrome, can cause misshapen or discolored teeth. Both the baby teeth and the permanent teeth are usually affected, particularly the eight front teeth and the six-year or first molars. Crowns may be pitted, grooved, and discolored.
Wisdom teeth
Wisdom teeth frequently have difficulty erupting because the jaw is too small. A wisdom tooth may rotate, tilt, or be displaced as it attempts to emerge, and it can become impacted (partially buried) in the gums. Impacted wisdom teeth do not always cause problems. However wisdom teeth are always difficult to clean and susceptible to decay and gum disease; thus an impacted wisdom tooth is usually extracted. An impacted tooth can cause:
- bad breath
- an unpleasant taste in the mouth
- gum pain
- recurrent infection of the tooth and surrounding gums
Parental concerns
Some evidence indicates that infants' jaws and teeth develop better and more completely if babies are fed breast milk rather than infant formula. To promote their baby's dental development, pregnant and nursing mothers should do the following:
- practice good nutrition
- refrain from prescription and nonprescription drugs, particularly during the first trimester of pregnancy
- refrain from alcohol, tobacco, and excessive sugar
Parents must clean and care for their children's teeth until children are able to do it themselves. Furthermore, parents are the first to teach their children good dental hygiene. After feeding, a baby's gums should be wiped with clean gauze. Brushing should begin with the first tooth eruption and the remaining gums should be cleaned and massaged. Flossing should begin as soon as all of the baby teeth have erupted.
When to call the dentist
The rapidity with which decay can advance in baby teeth necessitates periodic dental examinations and cleanings. Pediatric dentists often recommend a first dental appointment at 12 to 18 months of age. Some recommend a first appointment at six months. At the very least, a child should see a dentist by age two-and-a-half or when all of the baby teeth have erupted.
KEY TERMS
Abscess —A localized collection of pus in the skin or other body tissue caused by infection.
Bicuspid —Premolar; the two-cupped tooth between the first molar and the cuspid.
Calcification —A process in which tissue becomes hardened due to calcium deposits.
Calculus —Plural, calculi. Any type of hard concretion (stone) in the body, but usually found in the gallbladder, pancreas, and kidneys. They are formed by the accumulation of excess mineral salts and other organic material such as blood or mucus. Calculi (pl.) can cause problems by lodging in and obstructing the proper flow of fluids, such as bile to the intestines or urine to the bladder. In dentistry, calculus refers to a hardened yellow or brown mineral deposit from unremoved plaque, also called tartar.
Canines —The two sharp teeth located next to the front incisor teeth in mammals that are used to grip and tear. Also called cuspids.
Crown —The natural part of the tooth covered by enamel. A restorative crown is a protective shell that fits over a tooth.
Dentin —The middle layer of a tooth, which makes up most of the tooth's mass.
Enamel —The hard, outermost surface of a tooth.
Eruption —The process of a tooth breaking through the gum tissue to grow into place in the mouth.
Impacted tooth —Any tooth that is prevented from reaching its normal position in the mouth by another tooth, bone, or soft tissue.
Incisor —One of the eight front teeth.
Malocclusion —The misalignment of opposing teeth in the upper and lower jaws.
Molars —The teeth behind the primary canines or the permanent premolars, with large crowns and broad chewing surfaces for grinding food.
Occlusion —The way upper and lower teeth fit together during biting and chewing. Also refers to the blockage of some area or channel of the body.
Plaque —A deposit, usually of fatty material, on the inside wall of a blood vessel. Also refers to a small, round demyelinated area that develops in the brain and spinal cord of an individual with multiple sclerosis.
Premolar —Bicuspid; the two-cupped teeth between the first molars and the cuspids.
Wisdom teeth —The third molars at that back of the mouth.
Between two-and-a-half and six years of age is a critical period for dental development. Parents should regularly examine a child's teeth for signs of decay, crowdedness, or misalignment. A dentist should be consulted if any of the following occurs:
- A child has an inherited disorder that affects the teeth or jaws, such as a protruding or recessed lower jaw.
- Tooth eruption occurs at least a year sooner or later than normal.
- The baby teeth do not erupt properly or seem crowded.
- A baby tooth becomes loose before the age of four or five years.
- A permanent tooth begins to erupt before the baby tooth that it is replacing has been lost.
- Swelling or infection occurs during eruption of the molars.
- A child has difficulty chewing or closing their jaw.
- A child continues to thumb-suck or suck on a pacifier after all of the baby teeth have erupted.
- A child's diet contains excessive sugar.
- A child has a serious fall or blow to the head.
- A permanent tooth is loosened in an accident.
Parents should pay close attention to the child-dentist relationship and voice any concerns, since it is very important to prevent a child from having an unpleasant dental experience. Many parents choose to take their child to a pediatric dentist. A pediatric dentist has undergone additional training and may be more experienced with dental development in children. Their offices are usually designed specifically to make children feel comfortable.
See also Fluoridation ; Orthodontics .
Resources
BOOKS
Keller, Laurie. Open Wide: Tooth School Inside. New York: Henry Holt, 2000.
Nanci, Antonio. Ten Cate's Oral Histology: Development, Structure, and Function. St. Louis: Mosby, 2003.
Teaford, Mark F., et al., eds. Development, Function, and Evolution of Teeth. New York: Cambridge University Press, 2000.
PERIODICALS
Griffen A. L. "Normal Formation and Development Defects of the Human Dentition." Pediatric Clinics of North America 47, no. 5 (2000): 975–1000.
Macknin, M. L., et al. "Symptoms Associated with Infant Teething: A Prospective Study." Pediatrics 105, no.4 (2000): 747–52.
ORGANIZATIONS
American Academy of Pediatric Dentistry. 211 East Chicago Avenue, Suite 700, Chicago, IL 60611–2663. Web site: http://www.aapd.org.
American Dental Association. 211 East Chicago Avenue, Chicago, IL 60611–2678. Web site: http://www.ada.org.
National Maternal and Child Oral Health Resource Center (OHRC). Georgetown University, Box 571272, Washington, DC 20057–1272. Web site: http://www.mchoralhealth.org.
WEB SITES
"Early Childhood Tooth Decay (Baby Bottle Tooth Decay)." American Dental Association. Available online at http://www.ada.org/public/topics/decay_childhood_faq.asp (accessed December 10, 2004).
"A Health Professional's Guide to Pediatric Oral Health Management." National Maternal and Child Oral Heath Resource Center , 2004. Available online at http://www.mchoralhealth.org/PediatricOH/index.htm(accessed December 10, 2004).
"Tooth Eruption Charts." American Dental Association. Available online at http://www.ada.org/public/topics/tooth_eruption.asp (accessed December 10, 2004).
Margaret Alic, PhD
Comment about this article, ask questions, or add new information about this topic: