Abdominal wall defects
Definition
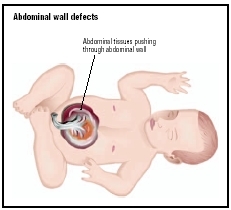
Abdominal wall defects are birth (congenital) defects that allow the stomach or intestines to protrude.
Description
Many unexpected events occur during the development of a fetus inside the womb. The stomach and intestines begin development outside the baby's abdomen and only later does the abdominal wall enclose them. Occasionally, either the umbilical opening is too large or it develops improperly, allowing the bowels or stomach to remain outside or squeeze through the abdominal wall. This results in one of two conditions, gastroschisis and omphalocele. Gastroschisis occurs when the abdominal wall does not close completely and the stomach and the small and large intestines appear outside the infant's body. In omphalocele, some of the internal organs protrude through the abdominal muscles in the area around the umbilical cord. Omphalocele may be minor, involving only a small portion of the intestines, or it may be severe with most of the abdominal organs, such as the intestines, liver, and spleen, outside the body.
Demographics
Abdominal wall defects, specifically gastroschisis and omphalocele, are rare and occur in only once in every 5000 births. Both boys and girls have these defects in equal numbers. While infants with gastroschisis rarely have defects other than those affecting the intestines, of children with omphalocele, 50 percent to 75 percent have associated congenital anomalies and 20 percent to 35 percent have chromosomal abnormalities.
Causes and symptoms
There are many causes for birth defects that still remain unclear. As of 2004, the causes of abdominal wall defects remained unknown. Any symptoms the mother may have had to indicate that the defects are present in the fetus are nondescript.
Diagnosis
At birth, the problem is obvious, because the base of the umbilical cord at the navel will bulge or, in worse cases, contain internal organs. Before birth, an ultrasound examination may detect the problem. It is always
Treatment
Abdominal wall defects are effectively treated with surgical repair. Unless there are accompanying anomalies, the surgical procedure is not overly complicated. However, if the defect is large, it may be difficult to fit all the organs into the small abdominal cavity.
Prognosis
If there are no other defects, the prognosis after surgical repair of this condition is relatively good. However, 10 percent of those with more severe or additional abnormalities die from it. The organs themselves are fully functional; the difficulty lies in fitting them inside the abdomen. The condition is, in actuality, a hernia requiring only replacement and strengthening of the passageway through which it occurred. However, after surgery, increased pressure in the stretched abdomen can compromise the function of the organs inside.
Prevention
Some, but by no means all, birth defects are preventable by early and attentive prenatal care, good nutrition , supplemental vitamins , and other elements of a healthy lifestyle, along with the diligent avoidance of all unnecessary drugs and chemicals—especially tobacco.
Parental concerns
Most children with abdominal wall defects require immediate and intensive medical care. Some of these infants may have multiple surgeries, and serious complications such as feeding problems and infections may persist long term. Parents will need to work closely with a team of physicians during the treatment of their child. Children with abdominal wall defects may need additional services, especially those with omphalocele and associated chromosomal abnormalities and birth defects. These children require long-term treatment for both the physical and developmental difficulties they face. Parents may need support services in addition to the services provided by the healthcare team. They can contact the hospital's social work department to learn more about available resources.
KEY TERMS
Congenital —Present at birth.
Hernia —A rupture in the wall of a body cavity, through which an organ may protrude.
Umbilical —Refers to the opening in the abdominal wall where the blood vessels from the placenta enter.
Resources
BOOKS
Key, Doneen. Do You Want to Take Her Home: Trials and Tribulations of Living Life as a Handicapped Person Due to Multiple Birth Defects. Lancaster, CA: Empire Publishing, 2001.
Moore, Keith L., et al. Before We Are Born: Essentials of Embryology and Birth Defects. Kent, UK: Elsevier, Health Sciences Division, 2002.
WEB SITES
"Birth Defects." National Center on Birth Defects and Developmental Disabilities. Available online at http://www.cdc.gov/ncbddd/bd/ (accessed October 15, 2004).
"Fetal Diagnoses: Omphalocele." The Center for Fetal Diagnosis and Treatment. Available online at http://www.fetalsurgery.chop.edu/omphalocele.shtml (accessed October 15, 2004).
"Gastroschisis." The Center for Fetal Diagnosis and Treatment. Available online at http://www.fetalsurgery.chop.edu/gastroschisis.shtml (accessed October 15, 2004).
J. Ricker Polsdorfer, MD Deborah L. Nurmi, MS
Thanks,
Jamie Appleberry